Arm and Cubital Fossa
1. On a skeleton and x-rays identify the coracoid process and acromion of the scapula, the greater and lesser tubercles [R373.1/2] of the humerus separated by the intertubercular groove, and the deltoid tuberosity [R373.7] (G11 6.1A, 6.31A & B, 6.47; G12 6.1A, 6.31A & B; N407A-B, 408A-B, 409). At the glenohumeral (shoulder) joint note the discrepancy in size between the large head of the humerus and the shallow glenoid cavity of the scapula, which makes the joint inherently unstable.
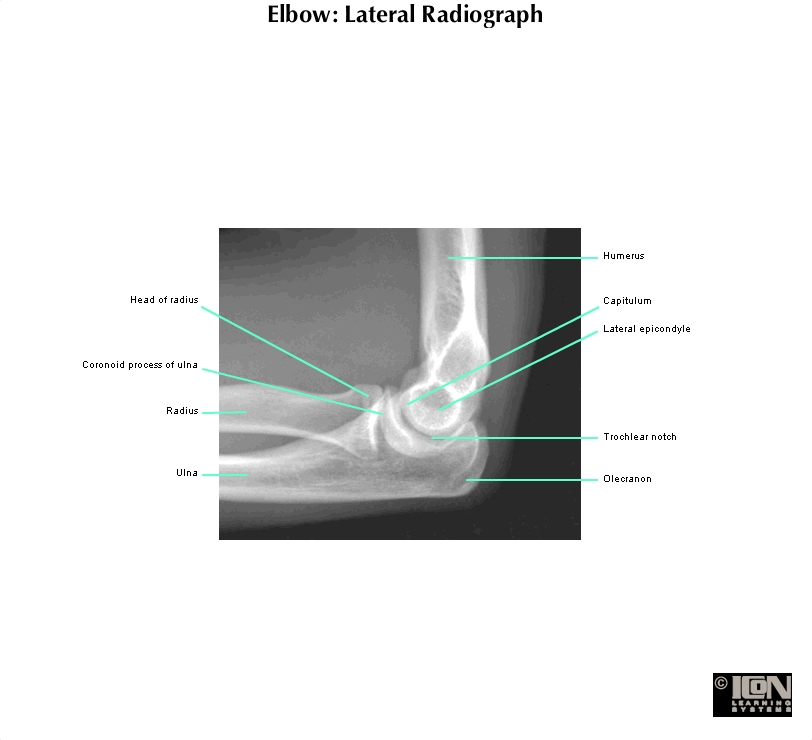
2. In the elbow region, find the medial and lateral epicondyles [R373.11/18], the trochlea, and the capitulum of the humerus; the olecranon, coronoid process, and tuberosity of the ulna; and the head,neck, and tuberosityof the radius (G11 6.31, 6.52; G12 6.31, 6.2C-D, 6.49C-D; N424A, B & C, 425A-B). Attempt to palpate these structures on the cadaver.
3. Make a shallow vertical incision through the skin down the middle of the anterior arm and continue inferiorly for 8-10 cm distal to the elbow. Make an incision encircling the forearm at the distal end of the first incision. Carefully reflect and remove the skin of the arm, leaving the superficial fascia intact.
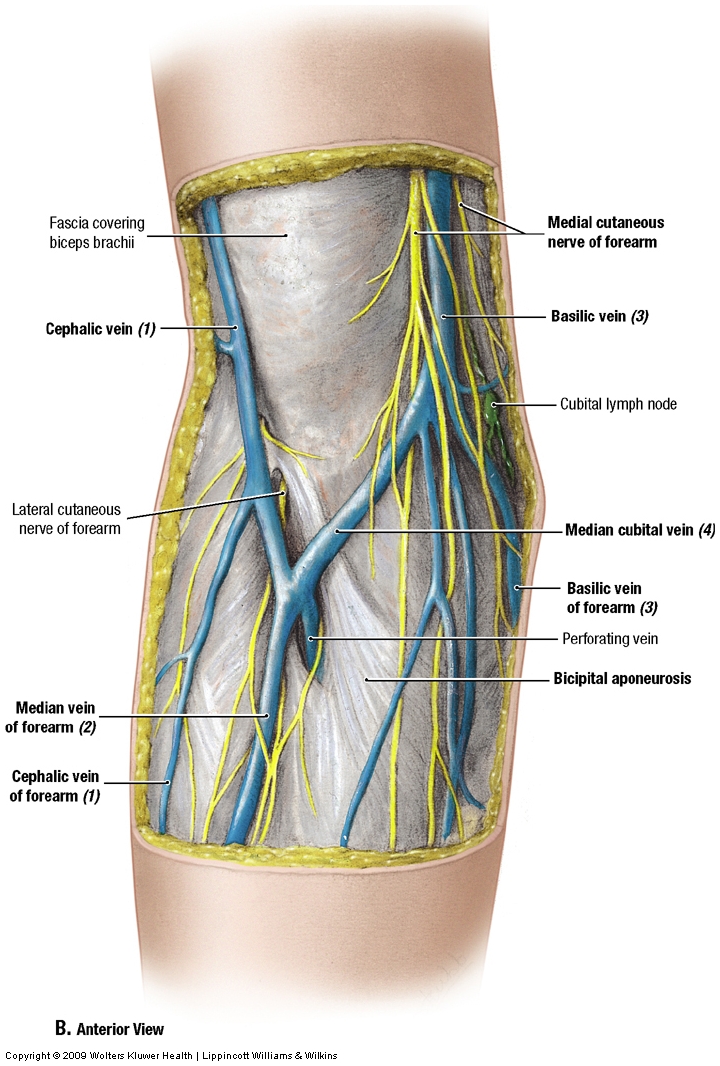
The cephalic vein ascends through the superficial fascia of the arm in a groove lateral to the biceps brachii (lateral bicipital furrow) and enters the deltopectoral triangle. The basilic vein ascends medial to the biceps (medial bicipital furrow) to just below the middle of the arm, where it penetrates the deep fascia of the arm, the brachial fascia (G11 6.6A & D, 6.7; G12 6.10A & D, 6.9; N403A-B). The two veins are joined across the front of the elbow (cubital fossa) in a variable manner by the median cubital vein (G11 6.49B; G12 6.45B; N403A-B), which often is used for venipuncture.
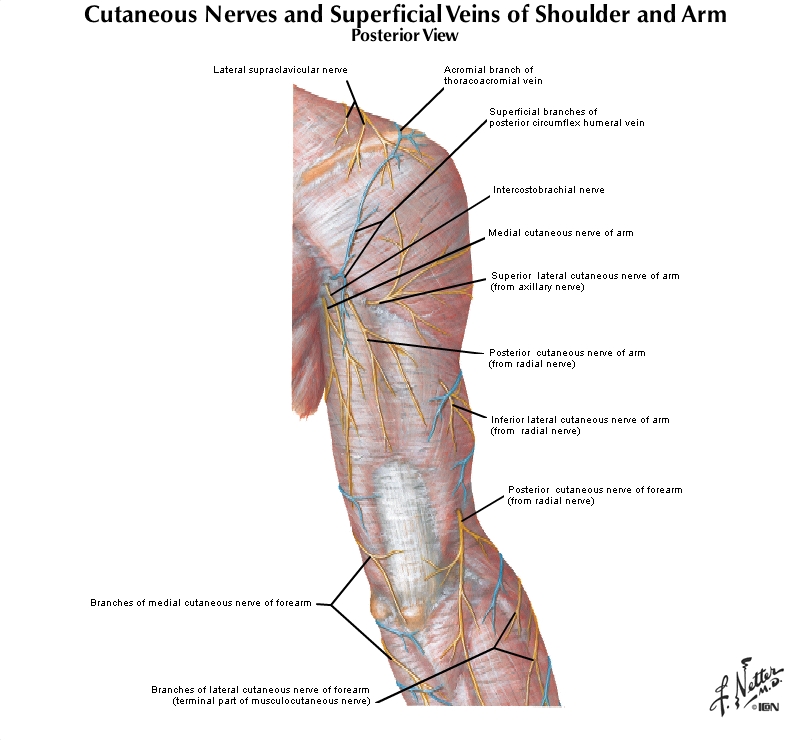
The medial brachial cutaneous nerve supplies skin on the medial side of the proximal arm (G11 6.4A; G12 6.6A; N403, 417). There is often a communication between the medial brachial cutaneous nerve and the intercostobrachial nerve from the second intercostal space. This is a pathway for referred pain from the heart to the medial side of the arm since the T1-2 spinal cord segments receive afferent input from both the heart and the skin of the medial arm. Heart pain is more commonly referred to the left arm but may be referred to the right arm.
The medial antebrachial cutaneous nerve emerges into superficial fascia of the arm where the basilic vein penetrates the deep fascia (G11 6.4A, 6.49B; G12 6.6A 6.45B; N403A-B, 404A-B). The medial brachial and medial antebrachial cutaneous nerves are branches of the medial cord of the brachial plexus.
The lateral antebrachial cutaneous nerve enters superficial fascia just lateral to the biceps brachii tendon, near its attachment into the radial tuberosity (G11 6.4A, 6.49B-C; G12 6.6A, 6.45B-C; N403A-B, 404A-B, 419A-B). The lateral antebrachial cutaneous nerve is the continuation of the musculocutaneous nerve from the lateral cord. Small branches of the superior and inferior lateral brachial cutaneous nerves may be found lateral to the cephalic vein, but these nerves usually are easier to dissect from the posterior side.
{kind=link}
The anterior compartment of the arm will now be studied. The arm is enclosed by deep fascia, the brachial fascia, which sends medial and lateral intermuscular septa to the lower half of the humerus (G11 6.10A, 6.92A & C; G12 6.32A, 6.90C; N423). The intermuscular septa and humerus divide the arm into anterior (flexor) and posterior (extensor) compartments. The three muscles in the anterior compartment of the arm are the coracobrachialis, biceps brachii, and brachialis, all innervated by the musculocutaneous nerve (C5,6,7) (G11 6.25, 6.34A, Table 6.6 [p. 500]; G12 6.26, 6.35A; N419, 421).
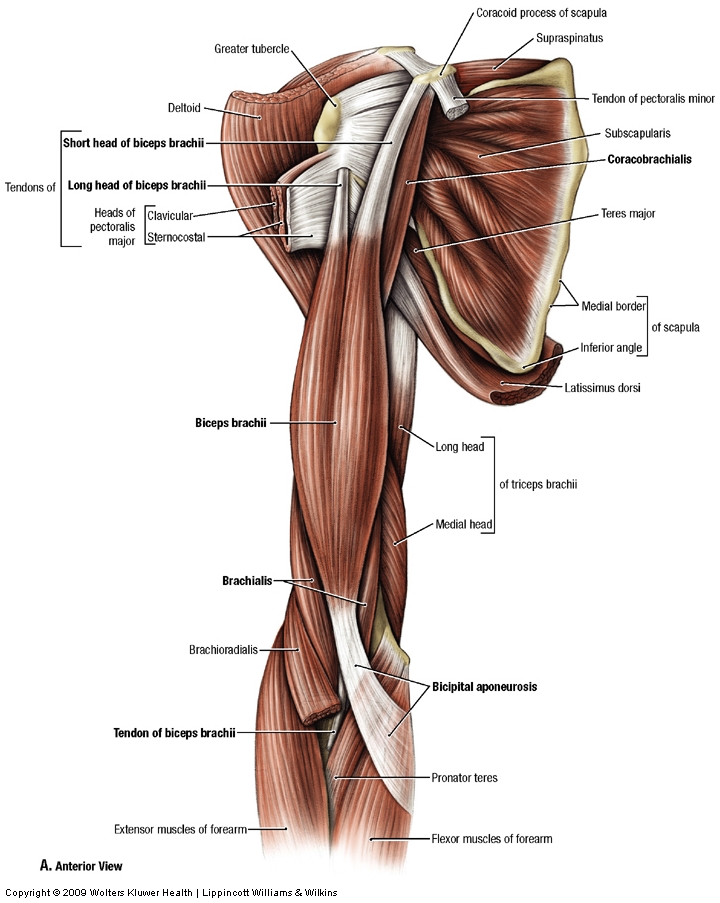
The coracobrachialis muscle is located in the superomedial part of the arm (G11 6.23, 6.25, 6.32, 6.33; G12 6.24, 6.26, 6.33A-B; N419, 421). It attaches proximally to the coracoid process of the scapula beside the short head of the biceps brachii, with which its origin is fused. The coracobrachialis inserts on the medial surface of the humerus, just above the middle of the shaft. The muscle is a useful landmark in the arm because it is usually pierced by the musculocutaneous nerve. The coracobrachialis helps to flex and adduct the arm.
The biceps brachii has short and long heads of proximal attachment (origin). The short head shares an attachment on the coracoid process with coracobrachialis (G11 6.23, 6.32; Table 6.6 [p. 500]; G12 6.24, 6.33A; N419, 421). The tendon of the long head of the biceps attaches to the supraglenoid tubercle of the scapula and traverses the cavity of the shoulder joint to descend in the intertubercular groove of the humerus (G11 6.43B, 6.46A; G12 6.43C; N410A&C, 419, 421). The long head is lateral to, and actually appears shorter than, the short head at this point in the dissection because most of it is hidden by other structures.
As the tendon of the long head of the biceps brachii traverses the joint cavity of the glenohumeral joint, it passes above the head of the humerus, which it helps to stabilize (G11 6.42, 6.43B, 6.45B; G12 6.42C, 6.43B). The tendon is enclosed by a layer of synovial membrane, which separates it from the synovial cavity of the joint; therefore, the tendon is inside the fibrous capsule of the joint but outside the synovial cavity (i.e., it is intracapsular but extrasynovial). This is an arrangement that we shall see also with the cruciate ligaments in the knee joint.
The two heads of the biceps brachii join to form the belly of the muscle, which has a tendon of distal attachment into the tuberosity of the radius. The bicipital aponeurosis is a flattened expansion of the biceps tendon that sweeps medially to blend with deep fascia of the forearm (antebrachial fascia) and functions as a muscle attachment (G11 6.32, 6.49; G12 6.33A, 6.45B-C; N419, 421). The biceps brachii flexes and supinates the forearm at the elbow joint. It also helps to flex the arm at the shoulder joint. Note that the biceps does not have an attachment on the humerus.
{kind=link}
{kind=link}
The brachialis muscle arises from the lower half of the humerus and the medial and lateral intermuscular septa and attaches distally to the coronoid process and tuberosity of the ulna (G11 6.33, Table 6.6 [p. 500]; G12 6.33B; N407, 419). The brachialis is the main flexor of the elbow joint, being active in all positions of the forearm.
The brachial artery is the continuation of the axillary artery at the lower border of the teres major muscle. It descends the medial bicipital furrow to the front of the elbow (cubital fossa) to divide into the radial and ulnar arteries (G11 6.11A & C, 6.34A; G12 6.7A & C, 6.35A; N421, 422). The brachial artery typically has two accompanying veins (venae comitantes, brachial veins) (G11 6.8, 6.19; G12 6.8A-B, 6.19; N417, 423). An important branch near the beginning of the brachial artery is the profunda brachii artery (deep artery of the arm), which enters the posterior compartment of the arm with the radial nerve (G11 6.11C, 6.22A, 6.25; G12 6.7C, 6.22C, 6.26; N420, 422). The profunda brachii has radial collateral and middle collateral branches that participate in the collateral circulation around the elbow joint.
The small superior ulnar collateral artery arises medially from the upper half of the brachial artery and descends with the ulnar nerve. The superior ulnar collateral artery and the ulnar nerve course posterior to the medial epicondyle of the humerus, where the superior ulnar collateral artery participates in the collateral circulation around the elbow joint (G11 6.11C, 6.34A; G12 6.7C, 6.35A, N421, 422). The inferior ulnar collateral artery branches from the brachial artery about 5 cm above the elbow. It descends anterior to the medial epicondyle to contribute to the collateral circulation. The collateral circulation around the elbow joint means that the brachial artery can be clamped surgically distal to the profunda brachii artery. What would happen if the axillary or brachial artery were clamped between the subscapular and profunda brachii arteries?
The median nerve descends through the arm with the brachial artery. The nerve first courses lateral to the artery, but near the midpoint of the arm it crosses in front of the artery to lie medial to it in the cubital fossa (G11 6.34A, 6.49C-D; G12 6.35A, 6.45C-D; N421, 434). The median nerve usually has no branches in the arm, but be aware of possible variations (e.g., fibers of the musculocutaneous nerve occasionally travel halfway down the arm with the median nerve and appear to branch from it to supply anterior compartment muscles).
The ulnar nerve descends from the medial cord of the brachial plexus to about the middle of the arm with the brachial artery (G11 6.34A; G12 6.35A; N421). There the nerve pierces the medial intermuscular septum with the superior ulnar collateral artery to enter the posterior compartment of the arm and descends between the septum and the medial head of the triceps brachii muscle. The ulnar nerve passes posterior to the medial epicondyle, where it is vulnerable to injury by being bumped (the “funny bone”) or in a fracture (G11 6.34, 6.36, 6.51B-C; G12 6.35A-B, 6.37, 6.47B, 6.48; N421, 432, 433).4. Bluntly dissect through the superficial fascia of the lateral and medial bicipital furrows to find the cephalic [R416.4] and basilic veins [R419.12], respectively. Remember that the basilic vein penetrates the deep fascia just below the middle of the arm. Where the basilic vein passes deep, find the medial antebrachial cutaneous nerve [R419.11]emerging into superficial fascia to descend into the forearm. Higher in the arm, look for the small medial brachial cutaneous nerve [R419.10]. Both the medial brachial cutaneous and the medial antebrachial cutaneous nerves are branches of the medial cord of the brachial plexus. Clean the lateral antebrachial cutaneous nerve [R420.4] entering superficial fascia anterior to the elbow, just lateral to the biceps brachii tendon [R420.2] (G11 6.49B-C; G12 6.45B-C; N403, 419). This nerve is the continuation of the musculocutaneous nerve.
5. Remove the brachial fascia over the anterior compartment of the arm. Clean the biceps brachii muscle and identify its long head [R415.14]. Most of the tendon of the long head of the biceps brachii is currently hidden from view, but find where it emerges from the intertubercular groove of the humerus deep to the transverse humeral ligament (G11 6.41; G12 6.42A; N410, 419). The short head of the biceps brachii [R411.5] arises from the coracoid process of the scapula.
6. Identify the coracobrachialis muscle arising from the coracoid process with the short head of the biceps brachii [R411.12] (G11 6.23, 6.32; G12 6.24, 6.33A; N419, 421). Follow the coracobrachialis to its attachment halfway down the medial surface of the shaft of the humerus. Note that the musculocutaneous nerve [R415.24] continues from the lateral cord of the brachial plexus and usually pierces the coracobrachialis to enter the fascial interval between the biceps [R415.14] and brachialis [R415.6] (G11 6.25; G12 6.26; N419). A smaller nerve entering the coracobrachialis proximal to the main trunk of the musculocutaneous nerve is a muscular branch. An occasional anatomical variation is that the musculocutaneous nerve travels midway down the arm with the median nerve and appears to branch from it to enter the anterior compartment. In this variation, the musculocutaneous nerve does not pierce the coracobrachialis, which receives only its usual small muscular branch.
7. Lift—DO NOT CUT!—the muscle belly of the biceps brachii to expose the underlying brachialis muscle [R415.16]. Clean the neurovascular structures in the medial bicipital furrow. Find where the profunda brachii artery [R415.13/21] branches from the brachial artery. Look for a small branch of the radial nerve, the ulnar collateral nerve, that accompanies the ulnar nerve [R419.21] and superior ulnar collateral artery [R419.22]. The ulnar collateral nerve passes to the medial head of the triceps brachii. Attempt to find another proximal branch of the radial nerve to the long head (G11 6.34A; G12 6.35A). Dissect the inferior ulnar collateral artery, which arises about 5 cm proximal to the elbow and descends anterior to the medial epicondyle (G11 6.34A, 6.49C; G12 6.35A, 6.45C; N421, 422).
CUBITAL FOSSA
8. On a skeleton and x-rays again identify the medial and lateral epicondyles, trochlea, and capitulum of the humerus;head, neck, and tuberosity of the radius; the coronoid process, tuberosity, radial notch, supinator crest and fossa, and theolecranon of the ulna; and the proximal radioulnar joint (G11 6.52A-C, 6.59; G12 6.2C & G, 6.49C, 6.56; N424A, B & C, 425A-B).
{kind=link}
9. The most advantageous position of the cadaver (i.e., prone or supine) for dissection of the cubital fossa varies from body to body depending on the position of the upper extremity and how flexible it is. If you are unsure how to best position the cadaver for this dissection, please ask an instructor.
10. Make an incision through the skin only in the middle of the anterior surface of the forearm as far as the wrist and reflect the skin flaps. The cephalic vein and the basilic vein were dissected in the superficial fascia of the arm. Continue cleaning them distally in the proximal half of the forearm (G11 6.6A & D, 6.49; G12 6.10A & D, 6.45; N400, 403A-B, 404A-B). Find the median cubital vein [R419.3] connecting the cephalic and basilic veins across the front of the elbow. It is frequently used for venipuncture. A median antebrachial vein [R419.8] may descend from the median cubital vein in the middle of the anterior forearm. As elsewhere in the body, the arrangement of superficial veins tends to be quite variable. Look for short perforating veins that carry blood from the superficial to the deep veins of the extremity,where the contractions of the surrounding muscles can help propel blood toward the heart (musculovenous pump).
11. The lateral and medial antebrachial cutaneous nerveswere dissected in the lower arm. Continue cleaning them distally in the proximal half of the forearm(G11 6.4A, 6.49; G12 6.6A, 6.45; N404A-B). The lateral antebrachial cutaneous nerve is the continuation of the musculocutaneous nerve where it emerges into superficial fascia lateral to the biceps brachii tendon. XXX
The cubital fossa is a depression on the anterior aspect of the elbow bounded medially by the pronator teres muscle, laterally by the brachioradialis muscle, and proximally by an imaginary line connecting the medial and lateral epicondyles of the humerus (G11 6.49C-D, 6.60; G12 6.45C-D, 6.57B; N421, 434). The floor is formed by the brachialis and supinator muscles. The central structure in the cubital fossa is the tendon of the biceps brachii muscle approaching its insertion at the radial tuberosity. A flattened band, the bicipital aponeurosis, leaves the medial side of the biceps tendon to fuse with the deep fascia of the forearm (antebrachial fascia) (G11 6.49B-C; G12 6.45B-C; N421, 434).
12. Cut and reflect the bicipital aponeurosis [R419.27] to expose the brachial artery [R420.3] and median nerve [R420.18] within the cubital fossa. Note that they lie medial to the biceps brachii tendon [R420.6]. The aponeurosis protects the artery and nerve during venipuncture of the median cubital vein. XXX
The brachial artery divides into its terminal branches, the radial and ulnar arteries, in the distal part of the cubital fossa (G11 6.11A & C, 6.49D, 6.58A, 6.61, Table 6.7 [p. 530]; G12 6.7A & C, 6.45D, 6.55B, 6.58B, 6.55A; N421, 422, 435). The radial artery leaves the cubital fossa superficial to the pronator teres muscle but is overlapped laterally by the brachioradialis. The ulnar artery exits the fossa by passing deep to the pronator teres muscle.
The median nerve leaves the cubital fossa between the superficial and deep heads of the pronator teres muscle (G11 6.49D; G12 6.45D, N434). As in other instances where a nerve passes through a muscle, the median nerve may be entrapped (compressed) by hypertrophy, inflammation, or fibrosis of the pronator teres muscle (pronator teres syndrome). The small deep head of the pronator teres occasionally is absent.
13. Clean the brachial artery and its division into the radial [R420.8] and ulnar arteries [R420.9] within the cubital fossa. Laterally, bluntly separate the origin of the brachioradialis muscle [R421.3] from the brachialis [R421.2] to expose the radial nerve [R421.4/5] (G11 6.49D, 6.61; G12 6.45D, 6.58B; N435). The radial nerve enters the anterior compartment of the arm just above the elbow by piercing the lateral intermuscular septum and its termination is traditionally described with the contents of the cubital fossa. Clean the division of the radial nerve into a superficial branch [R421.4] and a deep branch [R421.5]. The superficial branch of the radial nerve is a cutaneous nerve that descends through the forearm under the medial edge of the brachioradialis muscle. The deep branch pierces the supinator muscle to enter the extensor compartment of the forearm and will be seen again in the next dissection.
POSTERIOR COMPARTMENT OF THE ARM
For the next part of the dissection, the body should be in a prone position.
14. If the skin has not been removed over the posterior compartment of the arm, do so now. Find the superior(upper) lateral brachial cutaneous nerve [R405.20], a branch of the axillary nerve, which ascends across the deltoid from its posterior border (G11 6.4, 6.37; G12 6.6A-B, 6.38; N403A-B, 404A-B). Next, clean the inferior (lower) lateral brachial cutaneous nerve, a branch of the radial nerve, as it emerges into superficial fascia just inferior to the insertion of the deltoid muscle at the deltoid tuberosity. Slightly inferior to the inferior lateral brachial cutaneous nerve, find the posterior antebrachial cutaneous nerve entering superficial fascia en route to the forearm. Look for the posterior brachial cutaneous nerve [R405.24], also from the radial, as enters the upper part of the arm on its medial side (G11 6.4B, 6.34A; G12 6.6B, 6.35A; N403A-B).
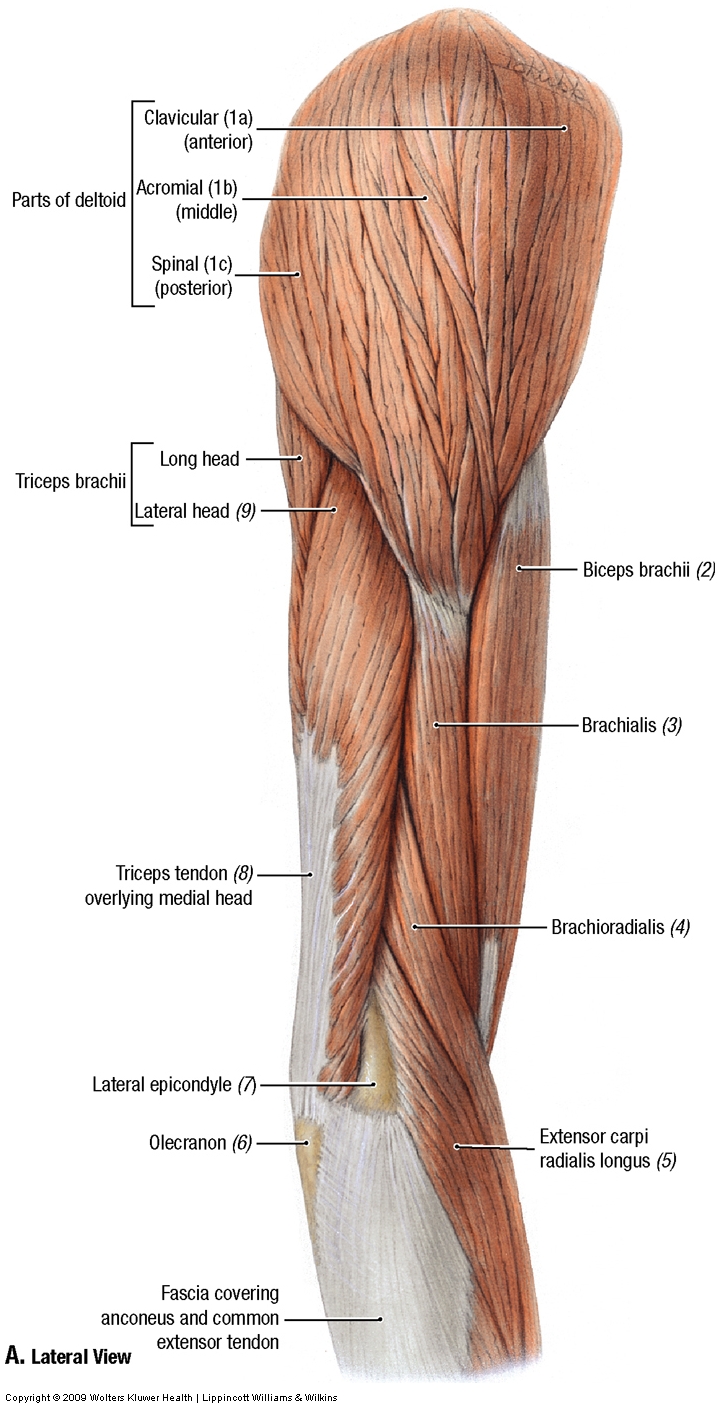
The posterior compartment of the arm contains one large muscle and one smaller muscle, both innervated by the radial nerve (G11 6.12C; G12 6.3C; N465). The main muscle is the triceps brachii, which has long, lateral, and medial heads (G11 6.35-6.38, Table 6.6 [p. 500]; G12 6.36, 6.37, 6.38, 6.34; N420). The long head of the triceps has already been seen descending from the infraglenoid tubercle of the scapula between the teres minor and teres major. The lateral and medial heads take origin from the shaft of the humerus superolateral and inferomedial, respectively, to the radial (spiral) groove (G11 6.31C-D, 6.36; G12 6.31D-E, 6.37; N408, 420). The three heads join to form a muscle belly with a tendon that inserts into the olecranon of the ulna. The triceps brachii extends the forearm. The long head also crosses the shoulder joint and helps to extend the flexed arm.
{kind=link}
The anconeus muscle passes from the lateral epicondyle of the humerus to the olecranon and upper posterior surface of the ulna (G11 6.51B, 6.76, 6.77B; Table 6.6 [p. 500]; G12 6.47B, 6.73, 6.74B; N420, 432). The anconeus is a small triangular muscle that helps the triceps brachii extend the elbow and may abduct the ulna during pronation of the forearm.
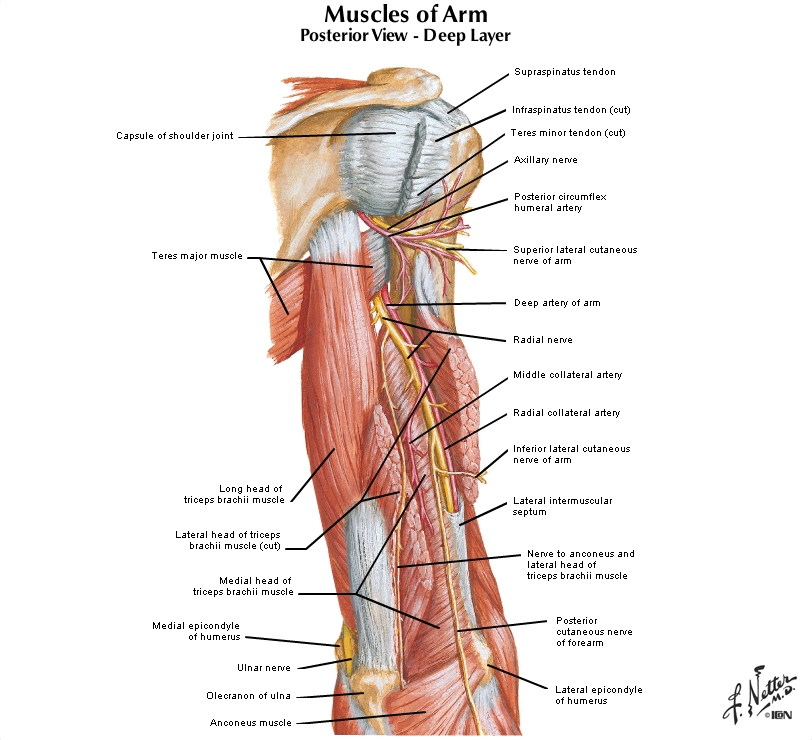
The nerve to the posterior compartment of the arm is the radial nerve. It enters the arm medial to the humerus and anterior to the long head of the triceps brachii, giving off branches to the long and medial heads of the triceps (G11 6.34A, 6.36; G12 6.35A, 6.37; N420). The branch to the medial head is the ulnar collateral nerve described above (G11 6.34A; G12 6.35A). The radial nerve descends to enter the radial (spiral) groove with the profunda brachii artery. In the radial groove the nerve gives off a branch to the lateral head and another to the medial head of the triceps.
{kind=link}
The radial nerve lies directly against bone in the radial groove of the humerus, where it is in danger during a fracture of the middle third (midshaft) of the humerus. Damage to the radial nerve at this location results in inability to extend the wrist (wristdrop). A midshaft fracture of the humerus does not eliminate elbow extension by the triceps brachii because of the branches to the medial head and the long head that leave the radial nerve before it enters the radial groove (G11 6.34A; G12 6.35A; N420).
The profunda brachii artery (deep artery of the arm) branches from the brachial artery high in the arm and courses posteriorly and laterally to enter the radial groove with the radial nerve (G11 6.25, 6.36; G12 6.26, 6.37; N420, 422). It is the principal blood supply to the triceps brachii. The profunda brachii artery terminates by dividing into middle and radial collateral arteries, which participate in the collateral circulation around the elbow (G11 6.11A & C, Table 6.7 [p. 530]; G12 6.7A & C, 6.55A; N422).15. Remove the brachial fascia over the posterior compartment of the arm and clean the triceps brachii muscle to its insertion into the olecranon of the ulna. Bluntly separate (i.e., pull apart) the long [R404.10] and lateral heads of the triceps brachii [R404.12] for several centimeters and identify the radial nerve [R404.21] and profunda brachii artery [R404.20] in the triangular interval between the two heads (G11 6.37; G12 6.38; N420 [upper]). Insert a probe into the triceps superficial to the nerve and artery to protect them and carefully cut and reflect the lateral head (G11 6.36; G12 6.37; N420 [lower]). This exposes the radial groove of the humerus with the radial nerve and profunda brachii artery traversing it. Identify and clean the nerve and artery. Palpate them to verify that they lie directly against the bone of the radial groove, where they may be injured by a fracture.
16. Identify the small anconeus muscle passing from the lateral epicondyle of the humerus to the olecranon and upper posterior surface of the ulna. XXX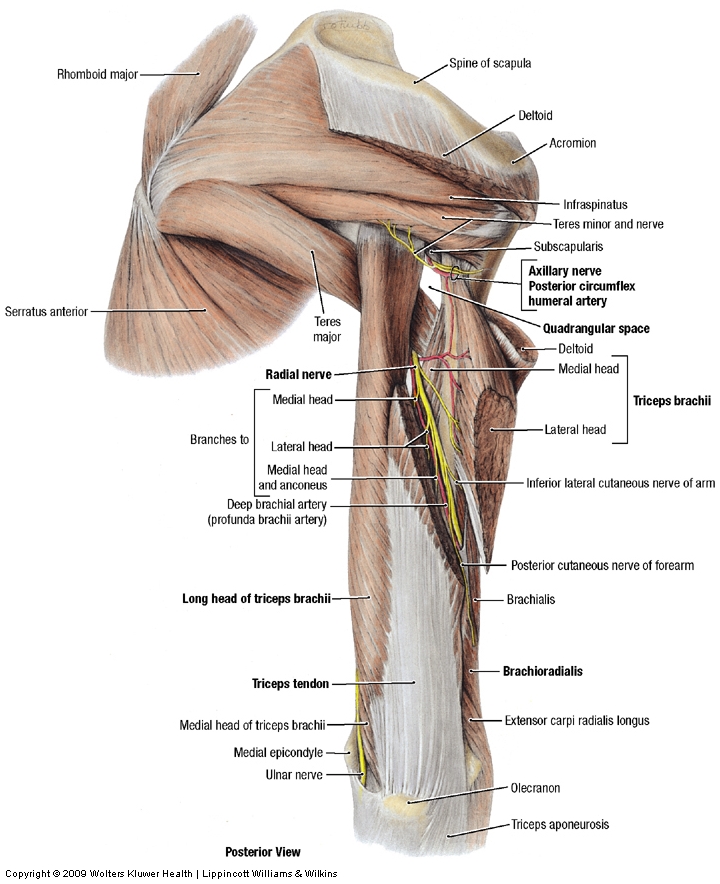{kind=link}
The illustrations in this dissection guide are used with permission from Gray’s Anatomy for Students. 2005, by Richard Drake, Wayne Vogel, and Adam Mitchell, Elsevier Inc., Philadelphia; and from Grant’s Atlas of Anatomy, 11E, 2005, Anne Agur and Arthur Dalley II, Lippincott Williams & Wilkins, Philadelphia.