Forearm, Wrist and Hand
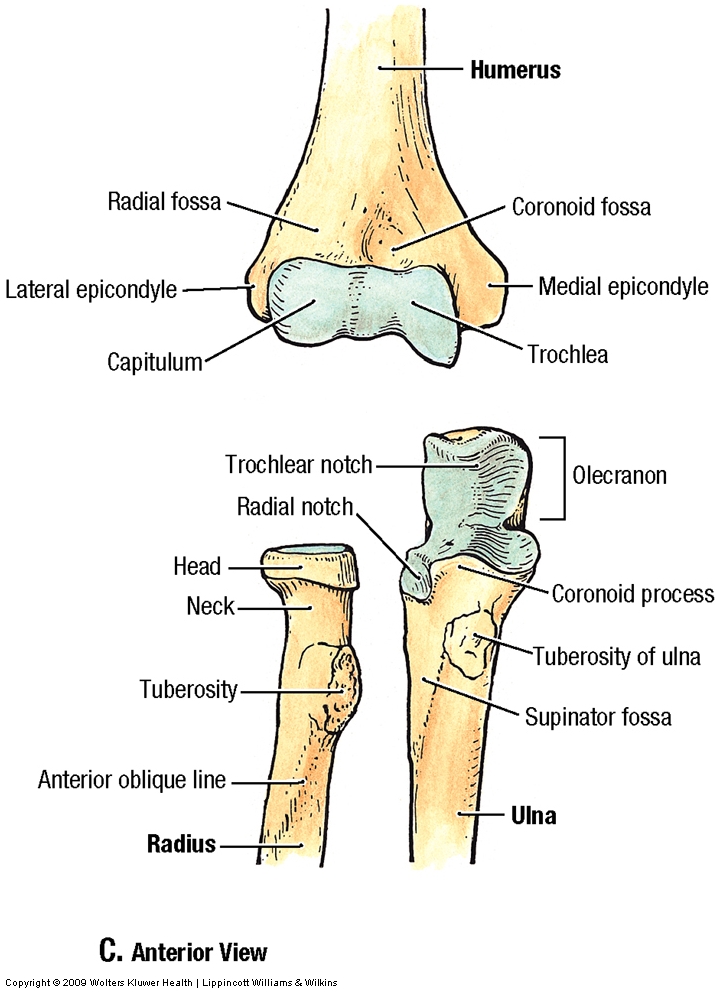
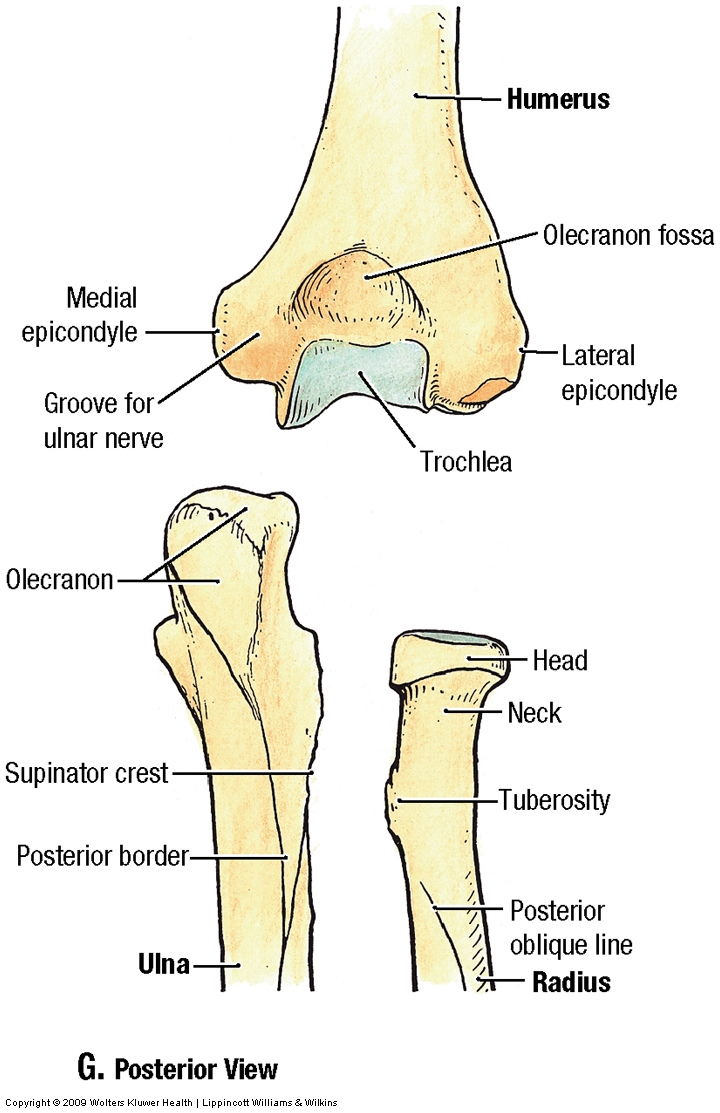
ANTERIOR FOREARM
During this period we will dissect the forearm, wrist, and hand.
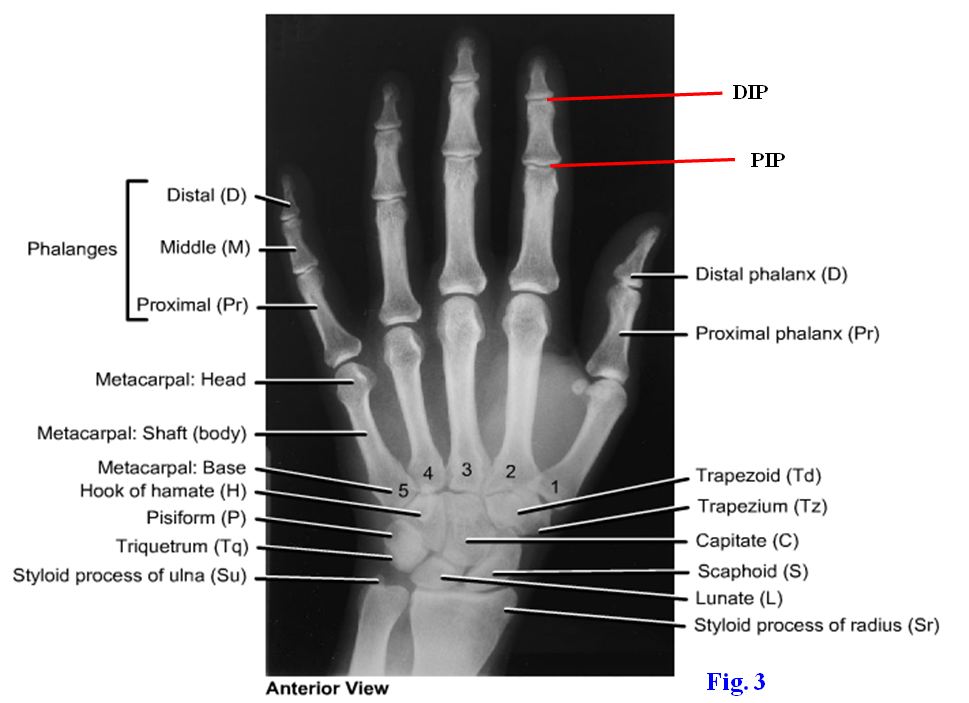
1. On a skeleton and x-rays identify thestyloid process and ulnar notch of the radius; the styloid process, head, and supinator crest and fossaof the ulna; the distal radioulnar joint; the radiocarpal (wrist) joint; and the individual members of the two rows of carpal (wrist) bones (G11 6.52A-B, 6.59, 6.84; G12 6.2C & G, 6.56A-B, 6.81A-B; N440A-B, 441A-B, 444A-B, 445). The proximal row of carpal bones consists of, from lateral to medial, the scaphoid, lunate, triquetrum, and pisiformbones (G11 6.83, 6.84; G12 6.80A-B, 6.81A-B; N440, 444). All except the pisiform bone articulate with the radius and articular disc at the radiocarpal joint. The distal row of carpal bones, from lateral to medial, comprises the trapezium, trapezoid, capitate, hamate. The distal row of carpal bones articulates with metacarpal bones at the carpometacarpal (CM) joints. Identify also the metacarpophalangeal (MP) and the proximal (PIP) anddistal (DIP) interphalangeal joints.
{kind=link}
{kind=link}
{kind=link}
The forearm is enclosed in deep fascia (antebrachial fascia) that blends medially with the ulna and laterally sends an intermuscular septum to the radius. The intermuscular septum, radius, interosseous membrane, and ulna divide the forearm into an anterior (flexor) compartment and a posterior (extensor) compartment.
2. If the skin has not been completely removed from the anterior surface of the forearm, do so now. Finish cleaning the cephalic vein and the basilic vein in the superficial fascia near the lateral and medial borders, respectively, of the forearm (G11 6.6A & D; G12 6.10A & D; N404A-B). Look for a median antebrachial vein descending in the middle of the forearm from the median cubital vein. As elsewhere in the body, the arrangement of superficial veins tends to be quite variable. Note perforating veins that carry blood from the superficial veins to the deep veins of the extremity.
3. Identify the proximal portions of the lateral and medial antebrachial cutaneous nervesbut don’t spend a lot of time cleaning them(G11 6.4; G12 6.6A-B; N404A-B). The former is the continuation of the musculocutaneous nerve where it emerges into superficial fascia lateral to the biceps brachii tendon. Laterally in the proximal forearm, briefly look for branches of the posterior antebrachial cutaneous nerve. Just above the wrist try to find the palmar cutaneous branches of the median and ulnar nerves.
4. Carefully remove the antebrachial fascia over the anterior compartment of the forearm. This may be difficult due to the attachment of the underlying muscle fibers to the fascia. XXX
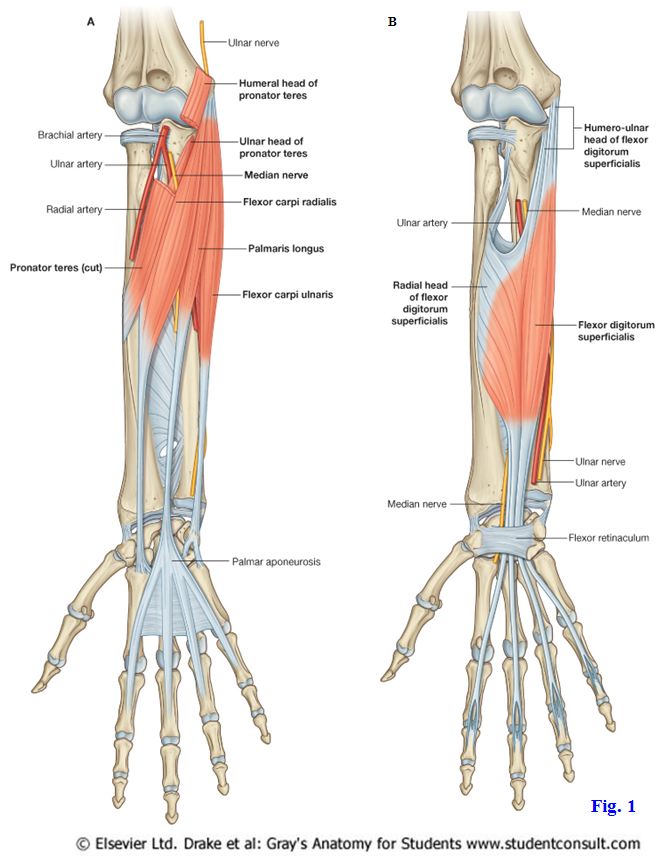
Most of the forearm muscles have proximal muscle bellies and slender distal tendons that enter the wrist and hand. The slender distal tendons plus the numerous small bones in the wrist and hand combine to allow relatively precise movements of the hand, especially the fingers. The muscles in the anterior compartment of the forearm flex the wrist and fingers and pronate the forearm. They are arranged in superficial, intermediate, and deep groups. The superficial group of forearm flexor muscles share a common proximal attachment (common flexor tendon) from the medial epicondyle of the humerus (Fig. 1A; G11 6.60, Table 6.8 [p. 533]; G12 6.10A & D, 6.55A; N434). From lateral to medial in the superficial group are the pronator teres, flexor carpi radialis, palmaris longus, and flexor carpi ulnaris.
The pronator teres has a superficial head from the medial epicondyle, which is easily identified, and a small deep head that is attached to the coronoid process of the ulna (G11 6.49; G12 6.45D; N428A-B, 435). The muscle descends laterally to insert into the middle of the lateral surface of the radius. The pronator teres assists the pronator quadratus in pronating the forearm when additional force or speed is needed. The median nerve enters the forearm between the superficial and deep heads of pronator teres (Fig. 1A; G11 6.49D; G12 6.45D; N435, 461), where it is in danger of becoming entrapped (pronator teres syndrome).
The flexor carpi radialis is a long fusiform muscle located just medial to the pronator teres. The muscle belly ends in the middle of the forearm in a long tendon that pierces the lateral part of the flexor retinaculum to attach into the base of the second metacarpal bone, and often the third (G11 6.60, 6.64C, 6.73, 6.74; G12 6.57B, 6.61C, 6.70, 6.71; N430, 434, 435). The flexor carpi radialis flexes and abducts the wrist.
The palmaris longus muscle has a small belly and a long, very slender tendon that is continuous with the palmar aponeurosis of the hand (Fig. 1A; G11 6.60; G12 6.57B; N434). This muscle is absent from one or both upper extremities in about 13% of the population (but, yes, there is still a palmar aponeurosis present if the palmaris longus is absent). When the palmaris longus is present, its tendon provides some protection against traumatic injury of the median nerve at the wrist (G11 6.64C; G126.61C; N434, 448A-B). The muscle tenses the palmar aponeurosis and helps to flex the wrist. The palmaris longus tendon sometimes is surgically removed for use in transplants.
The flexor carpi ulnaris is the most medial of the superficial flexor muscles (G11 6.60-6.63, 6.64C; G12 6.57B, 6.58B, 6.59B, 6.60B, 6.61C; N430, 434). It has an ulnar head of proximal attachment from the olecranon and posterior border of the ulna. The distal attachment is the hook of the hamate and the fifth metacarpal with the pisiform bone of the wrist classified as a sesamoid bone in the tendon of the flexor carpi ulnaris muscle. The flexor carpi ulnaris flexes and adducts the hand at the wrist. The ulnar nerve enters the forearm between the humeral and ulnar heads of flexor carpi ulnaris (cubital tunnel) (G11 6.51B-C; G12 6.47B, 6.48; N432, 433) and may become entrapped there in cubital tunnel syndrome (e.g., see http://www.emedicine.com/orthoped/TOPIC479.HTM ). The patient may experience weakened wrist flexion and adduction, weakened grip, and tingling (paresthesia) and numbness along the medial side of the hand and medial 1½ fingers.
5. Clean the short pronator teres [R420.19]. Sever its distal attachment at the radius and reflect the muscle medially. Identify the flexor carpi radialis [R420.20] and follow its tendon to the wrist. Notice that the flexor carpi radialis’ tendon is located just medial to the radial artery [R422.6] in the distal forearm, where an arterial pulse is commonly taken.
6. Demonstrate the presence or absence of a palmaris longus [R422.21] in your cadaver. If the muscle is present, note the relationship of the palmaris longus tendon to the median nerve. You may have to probe just lateral to the tendon to find the thick median nerve emerging from deep to the flexor digitorum superficialis, which will be dissected shortly (G11 6.60, 6.61; G12 6.57B, 6.58B; N434, 435).
7. Observe the most medial muscle of the superficial group, the flexor carpi ulnaris [R422.24]. The cubital tunnel formed between the humeral and ulnar heads of flexor carpi ulnaris is usually seen more easily from a posterior view (G11 6.51B-C; G12 6.47B, 6.48; N432, 433), so remember to look for it after dissecting the posterior compartment. XXX
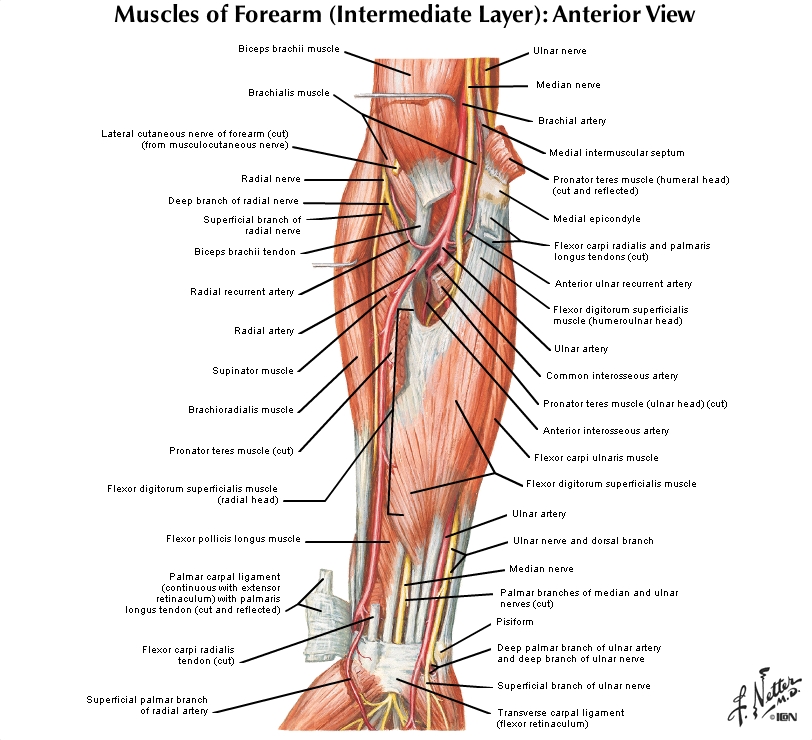
An intermediate layer of forearm flexor muscles is formed by a single muscle, the flexor digitorum superficialis (Fig. 1B; G11 6.61, Table 6.8 [p. 533]; G12 6.58B, Table 6.10 [p.553]; N431, 435). It shares an attachment from the medial epicondyle with the superficial group (humeroulnar head) and also has a radial head of attachment along the superior half of the anterior border of the radius. The muscle’s four tendons, one each to digits 2-5, traverse a confined space at the wrist, the carpal tunnel, to enter the palm of the hand (G11 6.71B-C, 6.94C-D; G12 6.68B-C, 6.92C-D; N449A-B, 450A-B). It will be seen later that each tendon splits over the proximal phalanx of its digit to allow passage of a flexor digitorum profundus tendon and then inserts into the sides of the middle phalanx (G11 6.62, 6.72B, 6.74; G12 6.59B, 6.69B, 6.71; N431, 452 [middle figure]). The flexor digitorum superficialis flexes the proximal interphalangeal (PIP) joints of digits 2-5 and can help to flex the metacarpophalangeal (MP) joints.
8. Trace each of the tendons of the flexor digitorum superficialis [R388.30] distally from the muscle belly to the carpal tunnel. Cut the radial attachment of the flexor digitorum superficialis (Fig. 1B; G11 6.61; G126.58B; N431, 435) and reflect it medially to expose the median nerve [R423.7] descending in the fascial interval between the flexor digitorum superficialis and the flexor digitorum profundus [R423.36]. Find the beginning of the ulnar artery [R423.20] as it descends medially to join the ulnar nerve [R423.13] under cover of the flexor carpi ulnaris (G11 6.61; G126.58B; N435). XXX
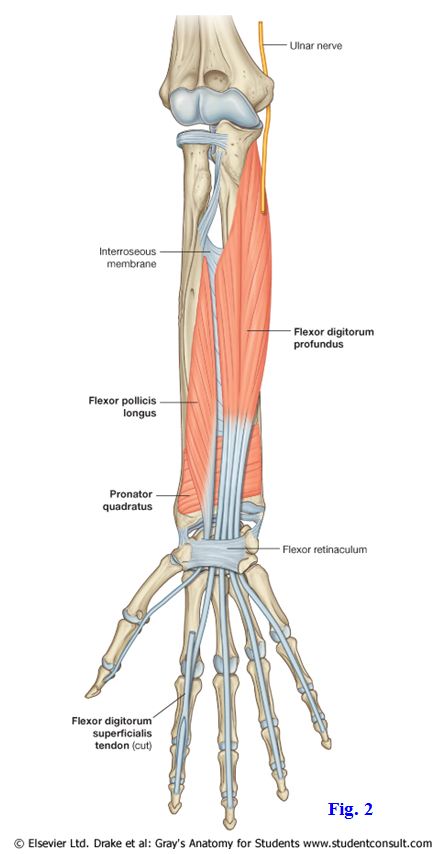
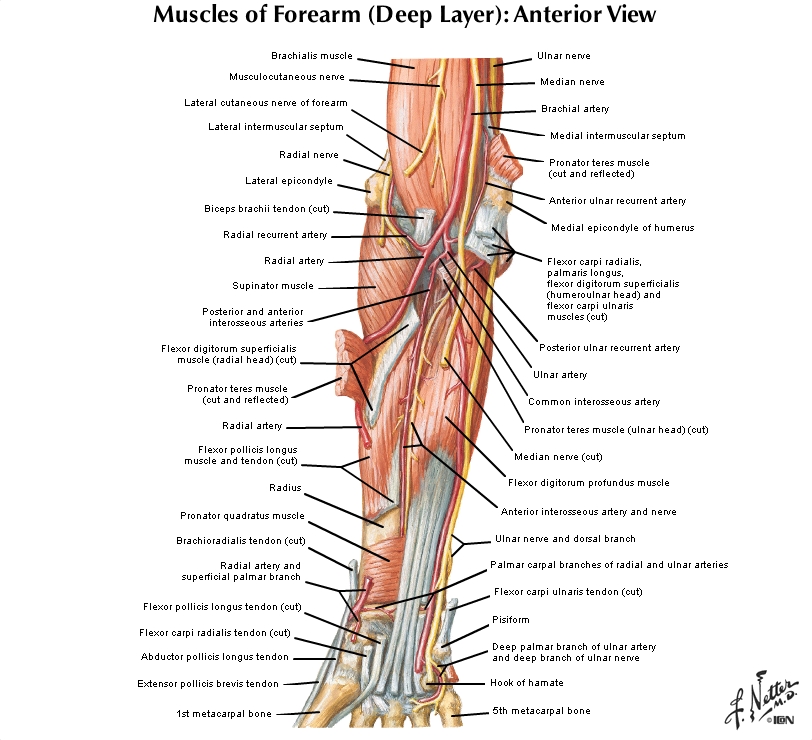
The deep layer of forearm flexor muscles comprises three muscles, none of which attach to the medial epicondyle of the humerus—the flexor digitorum profundus, flexor pollicis longus, and pronator quadratus (Fig. 2; G11 6.62, 6.63, 6.74; Table 6.8 [p. 533]; G12 6.59B, 6.60B, 6.71, Table 6.10 [p. 553]; N428A-B, 431, 436). All three receive innervation from the anterior interosseous branch of the median nerve, but the medial (ulnar) half of the flexor digitorum profundus, the part moving the fourth and fifth digits, is supplied by the ulnar nerve.
The flexor digitorum profundus attaches proximally to the ulna and interosseous membrane. Its four tendons descend from the muscle belly to enter the carpal tunnel deep to the tendons of flexor digitorum superficialis. In the palm the flexor profundus tendons give rise to lumbrical muscles, which pass to the dorsal surface of their respective digits (G11 6.70, 6.71C; G12 6.67B, 6.68C; N451A-B-C, 452A-B-C). In fingers 2-5 each flexor digitorum profundus tendon passes through a split in the corresponding flexor digitorum superficialis tendon to attach to the distal phalanx of its digit (G11 6.72B, 6.74; Table 6.8 [p. 533]; G12 6.69B, 6.71, Table 6.10 [p.553]; N431, 451A-B-C and 452A-B-C [middle figure]). The flexor digitorum profundus is the only muscle that can flex the distal interphalangeal (DIP) joints of fingers 2-5. Note that the long forearm muscles can help move more proximal joints as well as their primary joint of action (e.g., flexor digitorum profundus can flex not only the DIP joint, but also help with the PIP and MP joints of digits 2-5, although it cannot flex all of those joints through their full range of motion at the same time).
As the four tendons of flexor digitorum profundus traverse the carpal tunnel to enter the hand (G11 6.63, 6.94C-D; G12 6.60B, 6.92C-D; N449A-B, 450A-B), they share the common flexor synovial sheath (ulnar bursa) with the tendons of flexor digitorum superficialis muscle. Synovial sheaths, like bursae, are connective tissue sacs with smooth internal facing surfaces lubricated by a small amount of synovial fluid (G11 6.71, 6.72D; G12 6.68A-B-C, 6.69D; N448A-B, 452A-B-C). Synovial sheaths enclose tendons, allowing them to glide through confined spaces or over bone with minimum friction.
A synovial sheath may become inflamed (tenosynovitis), with edema and pain, and irritate or compress adjacent structures (e.g., nerves). There is a loss of range of motion. Chronic inflammation involving the tendon and tendon sheath may result in tendon rupture. For example, see http://www.merck.com/mmpe/sec04/ch040/ch040c.html#sec04-ch040-ch040b-806 Tendon rupture also may occur following a course of some antibiotics (e.g., fluoroquinolones, such as Levaquin) or steroid treatment. If inflammation results from infection, the infection may spread along a synovial sheath (e.g., from the little finger to the carpal tunnel at the wrist [G11 6.71B-C; G126.68B-C; N448A-B, 449A-B, 450A-B]).
The flexor pollicis longus is the second of the deep forearm flexor muscles. It lies lateral to the flexor digitorum profundus, passing from the anterior surface of the radius and interosseous membrane to the base of the distal phalanx of the thumb (Fig. 2; G11 6.62, 6.63, 6.71C; G12 6.59B, 6.60B, 6.68C; N431A-B, 435). As the tendon traverses the carpal tunnel, it has its own synovial sheath (radial bursa) lateral to the tendons of the flexor digitorum muscles (G11 6.71C, 6.94C-D; G126.68C, 6.92C-D; N449A-B, 450A-B). The flexor pollicis longus flexes the interphalangeal (IP) joint of the thumb and can help flex its MP joint.
9. Clean the flexor digitorum profundus [R423.36] muscle belly. Find its four tendons as they pass distally into the carpal tunnel deep to the flexor retinaculum [R423.8], where they lie deep to the tendons of flexor digitorum superficialis. Later, when the fingers are dissected, we will see that each flexor digitorum profundus tendon passes through a split in the corresponding flexor digitorum superficialis tendon to attach to the distal phalanx of its digit (Fig. 2, shown for index finger). Clean the muscle belly and tendon of the flexor pollicis longus [R423.39], which lies lateral to the flexor digitorum profundus. The flexor pollicis longus tendon passes through the carpal tunnel to the distal phalanx of the thumb. XXX
The pronator quadratus muscle passes transversely from the distal surface of the ulna to the distal surface of the radius deep to the tendons of the other forearm flexor muscles (G11 6.63, 6.71B, 6.74; G12 6.60B, 6.68B, 6.71; N428A-B, 436). The pronator quadratus is always active in pronation of the forearm but is assisted by the pronator teres when additional speed or force is needed.
10. Identify the transverse fibers of the pronator quadratus [R392.17]. This will require you to spread apart the tendons of the more superficial muscles. Take care not to damage any of the more superficial structures. XXX
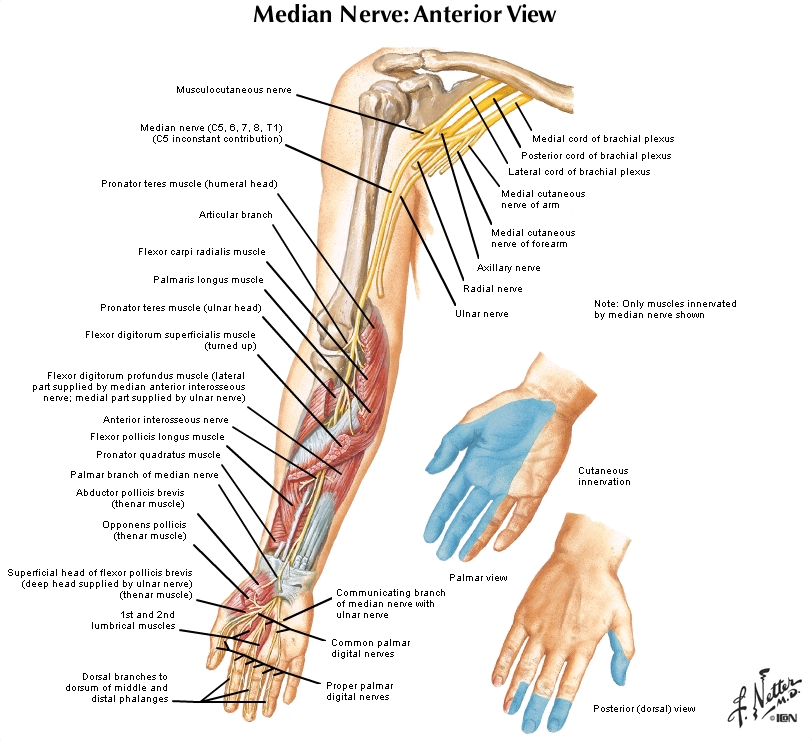
The median nerve descends through the forearm in the fascial interval between flexor digitorum superficialis and flexor digitorum profundus (G11 6.61, 6.62; G12 6.58B, 6.59B; N435, 463). The median nerve or its branches supply all of the muscles in the anterior compartment of the forearm except the flexor carpi ulnaris and the medial (ulnar) half of flexor digitorum profundus, which are innervated by the ulnar nerve. The anterior interosseous nerve branches from the median nerve in the proximal forearm to supply the three deep forearm flexor muscles (G11 6.62; G12 6.59B; N436). The anterior interosseous nerve may become entrapped (anterior interosseous syndrome), resulting in weakened pronation (pronator quadratus) with inability to flex the DIP joints of fingers two and three (flexor digitorum profundus) and the interphalangeal joint of the thumb (flexor pollicis longus).
{kind=link}
{kind=link}
{kind=link}
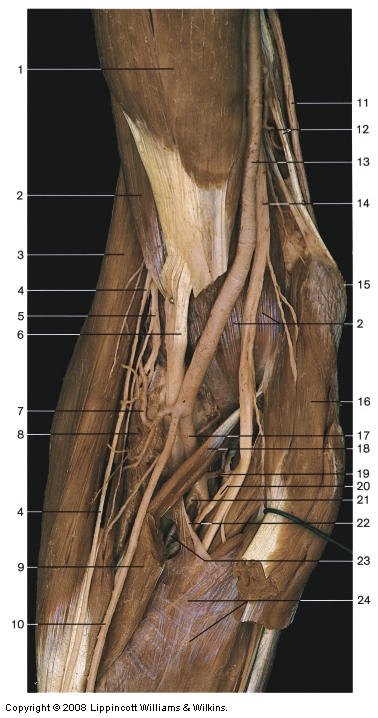
The ulnar nerve continues distally in the forearm from the cubital tunnel, which is located between the two head of the flexor carpi ulnaris. The nerve descends between the flexor carpi ulnaris and flexor digitorum profundus until just above the wrist, where it lies under the lateral edge of the flexor carpi ulnaris with the ulnar artery (Fig. 1; N435, 464).
11. Clean the median nerve as it descends between the flexor digitorum superficialis and flexor digitorum profundus muscles. Identify the anterior interosseous nerve [R421.20] branching from the median nerve in the proximal forearm. The anterior interosseous nerve passes deep between the flexor pollicis longus and flexor digitorum profundus and descends in the forearm on the anterior surface of the interosseous membrane with the anterior interosseous artery [R421.23](G11 6.63; G126.60B; N436). Look for the nerve and artery.
12. Follow the ulnar nerve as it descends in the forearm, first between the flexor carpi ulnaris and flexor digitorum profundus and then, just above the wrist, with the ulnar artery under the lateral edge of flexor carpi ulnaris (Fig. 1; G11 6.60-6.62; G12 6.57B, 6.58B, 6.59B; N434, 435, 436). At the wrist observe that the ulnar nerve and artery pass superficial to the flexor retinaculum [R422.20/27](i.e., not through the carpal tunnel) to enter the hand. The ulnar nerve innervates 1½ forearm muscles, the flexor carpi ulnaris and the medial (ulnar) half of flexor digitorum profundus. XXX
After branching from the brachial artery, the ulnar artery inclines medially to descend with the ulnar nerve (G11 6.62, Table 6.7 [p. 530]; G12 6.59B, 6.55A; N422, 436). Near its beginning the ulnar artery gives off the common interosseous artery, which quickly branches into an anterior interosseous artery and a posterior interosseous artery. The posterior interosseous artery passes into the posterior compartment above the interosseous membrane and gives rise to the interosseous recurrent artery (G11 6.58, 6.62, 6.63, Table 6.7 [p. 530]; G12 6.55A-B-C, 6.59B, 6.60B, 6.55A; N422, 433). The interosseous recurrent anastomoses with the middle collateral artery from the profunda brachii artery as part of the collateral circulation around the elbow (G11 6.11A & C, Table 6.7 [p. 530]; G12 6.7A & C, 6.55A; N422, 433).
The anterior interosseous artery descends along the anterior surface of the interosseous membrane with the anterior interosseous nerve. The artery pierces the interosseous membrane near the proximal edge of pronator quadratus to enter the posterior compartment of the forearm.
13. Again spread the flexor pollicis longus and flexor digitorum profundus apart and find the anterior interosseous artery and nerve descending on the interosseous membrane. Just proximal to the pronator quadratus muscle, the anterior interosseous artery pierces the interosseous membrane to enter the posterior compartment of the forearm (G11 6.58, Table 6.10, Lateral view [p. 553]; G12 6.55A-B-C, Table 6.12 [p. 573]; N433). Verify this. The posterior interosseous artery will be seen later.
14. Look for recurrent branches of the radial and ulnar arteries that participate in the collateral circulation around the elbow (G11 6.62, Table 6.7 [p. 530]; G12 6.59B, 6.55A; N422, 435, 436). The radial recurrent artery [R421.7]branches from the proximal portion of the radial artery and passes superiorly in front of the lateral epicondyle to anastomose with the radial collateral branch of the profunda brachii artery.
{kind=link}
15. The ulnar artery gives off the anterior ulnar recurrent artery [R421.19],which passes in front of the medial epicondyle to anastomose with the inferior ulnar collateral artery. The posterior ulnar recurrent artery, another branch of the ulnar artery, ascends behindthe medial epicondyle to meet the superior ulnar collateral artery. Clean these in one upper extremity. XXX
This collateral circulation (four sets of collateral and recurrent arteries) around the elbow is important when elbow flexion, traumatic injury, or surgical ligation impedes flow through the terminal part of the brachial artery. The branching points for arteries that participate in collateral circulation around a joint, such as the elbow, determine where the artery can be ligated without risking loss of the extremity due to ischemic necrosis of tissues. Loss of the arterial supply to the flexor compartment of the forearm is one cause of a compartment syndrome with Volkmann’s ischemic contracture (e.g., see http://www.emedicine.com/Orthoped/topic578.htm ) Would it be safe to ligate the brachial artery just proximal to the branching point of the profunda brachii (G11 6.11; G12 6.7A & C; N422)?
Study the relationships on the anterior aspect of the distal forearm and the wrist (G11 6.64; G12 6.61A-B-C; N434). These relationships are clinically important in lacerations (e.g., suicide attempts) and other injuries of the wrist. From lateral to medial are the tendon of abductor pollicis longus, radial artery, tendon of flexor carpi radialis, median nerve, tendon of palmaris longus (when present), tendons of flexor digitorum superficialis, ulnar artery, ulnar nerve, and tendon of flexor carpi ulnaris.
16. Identify these structures of the distal forearm on the cadaver. At the conclusion of lab, when your hands are clean, palpate on yourself and a lab partner the tendons of flexor carpi radialis, palmaris longus (if present), and flexor carpi ulnaris. Flexion of the wrist facilitates finding the tendons. Find the pulse of the radial artery just lateral to the flexor carpi radialis tendon. Try to feel the pulse of the ulnar artery, which may be hidden deep to the tendon of flexor carpi ulnaris. XXX
ANTERIOR WRIST AND PALM OF THE HAND.
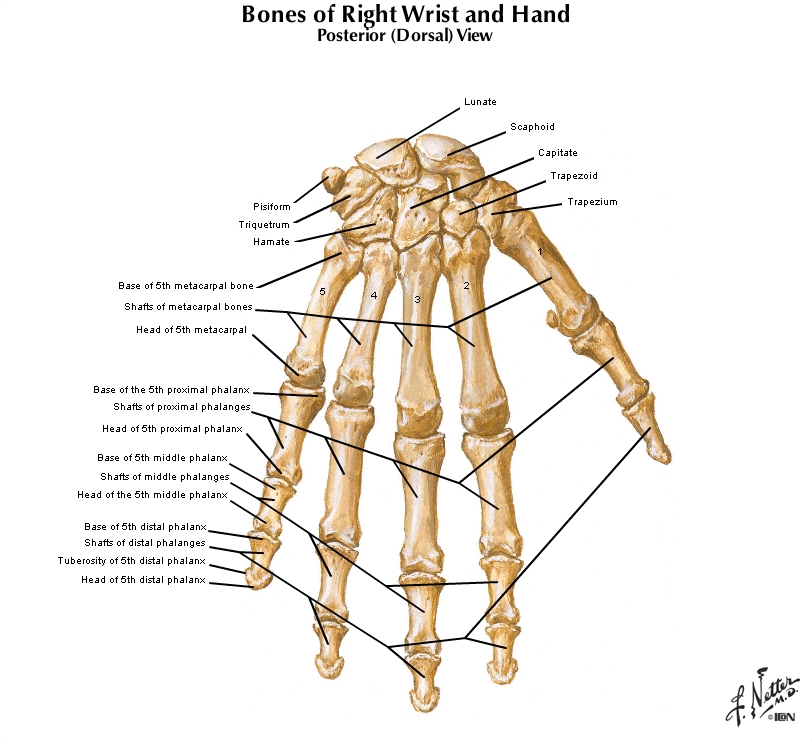
17. Study the osteology of the wrist and hand on a skeleton and on x-rays (Fig. 3; G11 6.59A, 6.83- 6.85; G12 6.56A-B, 6.80A-B, 6.81A-B, 6.82A-B; N444A-B, 445). The wrist consists of 8 carpal bones arranged in proximal and distal rows of four bones each. The proximal row of carpal bones is made up, from lateral to medial, of the scaphoid, lunate, triquetrum, and pisiform bones. The pisiform is often considered to be a sesamoid bone in the tendon of flexor carpi ulnaris. Find the tubercle of the scaphoid on the palmar surface of that bone.
18. The distal row of carpal bones comprises the trapezium, trapezoid, capitate, and hamate. Find the tubercle of the trapezium and the hook of the hamateon the palmar surface of those bones. Study the articulated carpal bones. Notice that they form a ventral concavity. This concavity is bridged in an intact body by the flexor retinaculum (transverse carpal ligament) to form the carpal tunnel (Figs. 1B, 2).
19. Examine the five metacarpal bones. Each consists of a proximal base, shaft (body), and distal head(Fig. 3; G11 6.84A; G126.81A; N444A-B). The metacarpal bone of the thumb is shorter and thicker than the other metacarpals and articulates with the trapezium at a sellar (saddle-shaped) joint (G11 6.89; G12 6.86A-B; N440, 441A-B), which allows its wide range of movements. The thumb differs from digits 2-5 also by having only two phalanges—proximal and distal—articulating at an interphalangeal (IP) joint. The other digits have three phalanges each—proximal, middle, and distal—articulating at proximal (PIP) and distal (DIP) interphalangeal joints (Fig. 3; G11 6.83, 6.84; G12 6.80A-B, 6.81A-B; N444A-B, 445). Each phalanx features a base, shaft, and head.
20. Position the cadaver’s hand so that you have access to the anterior side of the wrist and the palm. It may be necessary to gently pry open flexed fingers to gain exposure. Sometimes flexing the wrist helps with this movement. Palpate the pisiform bone, hook of the hamate, and the tubercle of the scaphoid bone in the wrist. Note that these wrist bones are in a region that many lay people consider part of the “hand.” XXX
The palm of the hand is subdivided into a central compartment covered superficially by the thick palmar aponeurosis, a medial hypothenar compartment covered by thin hypothenar fascia, and a lateral thenar compartment covered by thin thenar fascia (G11 6.66; G12 6.63; N447). The hypothenar compartment contains intrinsic hand muscles that move the little finger, and the thenar compartment contains intrinsic hand muscles that move the thumb. In the small fat pad superficial to the hypothenar fascia a small group of transversely oriented muscle fibers courses laterally from the palmar aponeurosis as the palmaris brevis muscle (G11 6.69; G12 6.67A; N447).
Deep to the central compartment of the palm is the interosseous-adductor compartment, which contains the adductor pollicis muscle and the palmar and dorsal interosseous muscles (G11 6.67A, 6.95; G12 6.64A, 6.93A-B; N450 [lower figure]). The deep palmar arch and deep branch of the ulnar nerve also are present. These will be studied after the more superficial structures of the palm.
21. Make a skin incision straight down the anterior surface of the wrist and palm, continuing down the middle of the third digit to the tip. The thick skin of the central palm is adherent to the underlying fibrous deep fascia of the palmar aponeurosis [R422.29] (G11 6.60, 6.66; G12 6.57B, 6.63; N447). Be careful not to cut into the aponeurosis. Make a transverse skin incision across the palm just proximal to the metacarpophalangeal (MP) joints. Also make an incision down the middle of the thumb to its tip. Remove the skin from the hand.
22. Clean the triangular palmar aponeurosis, which is continuous with the palmaris longus tendonwhen that muscle is present. Follow the longitudinal digital bands of the palmar aponeurosis to the base of fingers 2-5. Between the digital bands look for the distal portions of common palmar digital nerves and arteries (G11 6.66, 6.69, 6.75A; Table 6.10 [p. 553]; G12 6.63, 6.67A, 6.72A, Table 6.12 [p. 573]; N447, 454A-B). The proximal portions of these nerves and arteries are protected deep to the aponeurosis. Look medial and lateral to the edges of the palmar aponeurosis for other cutaneous branches of the ulnar and median nerves, respectively.
23. Use a probe to separate the distal portion of the palmar aponeurosis from underlying structures. Make a transverse cut across the distal end of the aponeurosis, preserving the cutaneous nerves and vessels. Reflect the palmar aponeurosis in a proximal direction to the tendon of the palmaris longus. If the palmar aponeurosis can’t be reflected intact, carefully remove it. XXX
The palm of the hand receives a rich blood supply via two palmar arterial arches (G11 6.69, 6.73, 6.75; Table 6.10 [p. 553]; G12 6.67A, 6.70, 6.72A-B, Table 6.12 [p. 573]; N448, 453, 454A-B). The superficial palmar arch is the direct continuation of the ulnar artery. The ulnar artery passes anterior to the flexor retinaculum and through the depression between the pisiform bone and hook of the hamate (Guyon’s canal) with the ulnar nerve. The artery divides into superficial and deep branches, and the larger superficial branch becomes the superficial palmar arch.
The superficial palmar arch passes radially across the palm deep to the palmar aponeurosis but superficial to the long flexor tendons (G11 6.69; G12 6.67A; N448). It is located distally about midlength of the metacarpal bones. The superficial arch may be completed laterally by a small superficial palmar branch of the radial artery. The superficial palmar arch gives off common palmar digital arteries, which in turn divide into proper palmar digital arteries to the adjacent sides of fingers (G11 6.75A; Table 6.10 [p. 553]; G12 6.72A, Table 6.12 [p. 573] N454A-B).
The deep palmar arch crosses the palm deep to the long flexor tendons and will be studied later.
24. Clean the superficial palmar arch [R428.23] (G11 6.69, 6.75, Table 6.10; G12 6.67A, 6.72A-B, Table 6.12 [p. 573]). Look to see if it is completed laterally by the superficial palmar branch of the radial artery [R428.8]. Clean common palmar digital arteries [R428.5] leaving the superficial palmar arch and dividing into proper palmar digital arteries [R428.27]. Identify common palmar digital nerves [R428.12] , which are branches of the median and ulnar nerves, accompanying the corresponding arteries (G11 6.69, 6.79; G12 6.67A, 6.76; N454A-B). Clean their division into proper palmar digital nerves [R428.14]. Note that the ulnar nerve provides cutaneous innervation to the medial 1½ digits and the median nerve to the palmar surface of the lateral 3½ digits (G11 6.4; G12 6.6A-B; N460).
25. Find the recurrent branch of the median nerve as it enters the thenar compartment (G11 6.64, 6.68, 6.69; G12 6.61A-B-C, 6.65, 6.67A; N447, 448, 454A-B, 461). This important nerve, which is motor to the intrinsic muscles of the thumb, is vulnerable to lacerations due to its superficial position in the palm. XXX
The flexor retinaculum (transverse carpal ligament) is a strong band of fibrous connective tissue spanning the ventral concavity created by the articulated carpal bones to form the carpal tunnel (Fig. 6-2, G11 6.62, 6.70, 6.74, 6.94C-D; G12 6.59B, 6.67B, 6.71, 6.92C-D; N435, 442A-B, 449A-B). The retinaculum prevents bowstringing of the long forearm flexor tendons during wrist flexion. Note that the ulnar nerve and artery and the tendon of palmaris longus pass superficial to the flexor retinaculum and that the median nerve and most long flexor tendons pass deep to the retinaculum through the carpal tunnel (G11 6.94C-D; G12 6.92C-D; N449A-B). 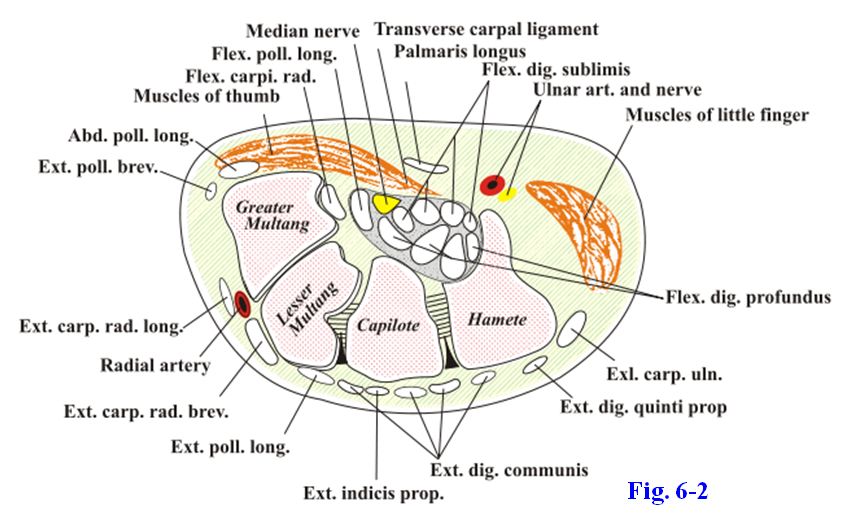
The carpal tunnel is a confined space with rigid walls, and any condition that significantly reduces the volume of the carpal tunnel (e.g., inflammation of the synovial sheaths due to repetitive motion or infection) may compress the median nerve. This carpal tunnel syndrome is a relatively frequent condition. It is characterized by pain and/or paresthesia, often worse at night, along the palmar surface of the lateral 3½ digits, sometimes radiating proximally into the forearm. In severe cases, there is loss of strength (paresis) and atrophy of the thenar compartment muscles with loss of precise thumb movements. See http://www.emedicine.com/EMERG/topic83.htm
26. Be aware of, but don’t spend a lot of time searching for, palmar cutaneous branches of the median and ulnar nerves branching in the distal forearm and entering the palm superficial to the flexor retinaculum. Clean the flexor retinaculum and study its attachments. Pass a probe deep to the flexor retinaculum to protect the contents of the carpal tunnel and incise the retinaculum vertically. Clean the median nerve as it traverses the carpal tunnel to reach the palm and follow its branches. If you didn’t see it previously, find the recurrent branch of the median nerve branching just distal to the flexor retinaculum. Occasionally it pierces the retinaculum.
27. Note the filmy synovial sheath (ulnar bursa) [R392.27] that envelops the tendons of the flexor digitorum superficialis and flexor digitorum profundus muscles within the carpal tunnel (Fig. 6-2; G11 6.71B-C, 6.94D; G12 6.68B-C, 6.92D; N448A-B, 449A-B, 450A-B). The tendons of the flexor digitorum superficialis are located superficial to those of the flexor profundus with the superficialis tendons that are destined for the middle and ring fingers positioned anterior to those of the index and little fingers. Be aware, although it is difficult to demonstrate in the dissection lab, that the ulnar bursa continues into the little finger but not into the other fingers. This is clinically important in the spread of infection. Try to find the radial bursa [R392.28] enclosing the tendon of flexor pollicis longus. Don’t attempt to demonstrate the individual digital synovial sheaths [R392.29] enclosing the long flexor tendons in the index, middle, and ring fingers (Fig. 6.71C; N450A-B and 451A-C [upper figure]).
28. Follow the flexor digitorum superficialis and profundus tendons through the palm into the middle finger. Incise the fibrous digital sheath [R394.44] to expose the tendons in a finger (G11 6.71A & C, 7.72C-D; G12 6.68A-C, 6.69C-D; N448A-B, 450A-B). The flexor digitorum superficialis tendon [R394.43] splits to allow the flexor digitorum profundus tendon [R394.42] to pass to the distal phalanx for its attachment (G11 6.62, 6.72B; G12 6.59B, 6.69B; N450A-B, 451A-B, 452A-C). Lift the tendons in the finger and look for delicate folds of synovial membrane, the vincula longa and brevia [R394.16/18/20], which carry blood vessels to the tendons (G11 6.72B; G12 6.69B; N452A-C).
29. In the palm find the lumbrical muscles [R389.41] at their origin from the flexor digitorum profundus tendons [R389.42] and clean them as they pass distally lateral to the metacarpophalangeal (MP) joints to insert into extensor expansions (G11 6.70, 6.71C, 6.72B, Table 6.9 [p. 545]; G12 6.67B, 6.68C, 6.69B, 6.66D, 6.76D; N451A-B, 452A-B-C). The first and second lumbrical muscles, which go to the index and middle fingers respectively, are innervated by the median nerve (G11 6.70; G12 6.67B; N454A-B). The third and fourth lumbricals go to the ring and little fingers, respectively, and are innervated by the ulnar nerve. XXX
The thenar and hypothenar compartments both contain a short abductor and a short flexor muscle that attach on the proximal phalanx of its digit (thumb and little finger, respectively) and an opponens muscle that inserts on the metacarpal bone. Start with the thenar compartment. The two superficial thenar muscles are the flexor pollicis brevis and abductor pollicis brevis (G11 6.69, Table 6.9 [pp. 544-545]; G12 6.67A, 6.66D, 6.76D; N453A-B-C, 454A-B, 463). The flexor takes origin from the flexor retinaculum and the tubercle of the trapezium. The abductor takes origin from the flexor retinaculum and the tubercle of the scaphoid. The flexor pollicis brevis flexes the carpometacarpal (CM) and the metacarpophalangeal (MP) joints, and the abductor pollicis brevis abducts the carpometacarpal (CM) joint of the thumb.
Deep to the abductor pollicis brevis is the opponens pollicis (G11 6.70; G12 6.67B; N453A-B-C), which performs the important movement of opposition of the thumb. During opposition the pad of the thumb is brought into contact with the pad of another finger. Opposition is a component of many activities and is estimated to be responsible for as much as 80% of the usefulness of the hand. The thumb is so important that the great toe may be transplanted or the index finger may be mobilized and re-positioned in an attempt to partially replace the function of an amputated thumb.
The recurrent branch of the median nerve innervates the muscles of the thenar compartment. An inconstant deep head of the flexor pollicis brevis usually is innervated by the deep branch of the ulnar nerve when the deep head is present, but for testing purposes, the innervation of thenar compartment muscles is the recurrent branch of the median nerve.
30. Clean the flexor pollicis brevis [R394.25] and abductor pollicis brevis [R394.24]. Cut the proximal attachment of the abductor pollicis brevis from the tubercle of the scaphoid and flexor retinaculum and reflect it toward the thumb to expose the underlying opponens pollicis muscle [R394.22](G11 6.70; G12 6.67B; N453A-B-C). The opponens is easy to distinguish because it inserts on the first metacarpal bone rather than the base of the proximal phalanx. Again find the recurrent branch of the median nerve entering the thenar compartment. Does the superficial palmar branch of the radial artery traverse the compartment to contribute to the superficial palmar arch? XXX
Turn your attention to the hypothenar compartment. The abductor digiti minimi passes to the little finger from the pisiform bone, and the flexor digiti minimi brevis reaches it from the flexor retinaculum and hook of the hamate (G11 6.70, 6.71C; Table 6.9 [p. 545]; G12 6.67B, 6.68C, 6.66D, 6.76D; N453A-B-C [upper figure], 464). The two muscles insert together on the medial side of the proximal phalanx of the little finger at its base. The flexor is variable in size and may be absent. The deep branches of the ulnar nerve and artery enter the hypothenar compartment between the abductor digiti minimi and flexor digiti minimi brevis.
The third muscle in the hypothenar compartment is the opponens digiti minimi. It lies deep to the abductor and flexor, passing from the flexor retinaculum and hook of the hamate to the fifth metacarpal bone.
31. Clean the abductor digiti minimi [R394.25] and flexor digiti minimi brevis [R394.36]. In one hand cut the flexor digiti minimi brevis near its proximal attachment and reflect it distally to expose the opponens digiti minimi passing to the shaft of the fifth metacarpal bone (G11 6.73; G12 6.70; N453A-B-C). Find the deep branch of the ulnar nerve as it branches from the ulnar nerve in the osseofibrous tunnel between the pisiform and the hook of the hamate, Guyon’s canal (G11 6.70, 6.73; G12 6.67B, 6.70; N448A-B, 464). XXX
The ulnar nerve may be compressed by any space-occupying lesion (e.g., a ganglion cyst) in Guyon’s canal (for example see http://www.emedicine.com/Orthoped/topic574.htm ).
The adductor pollicis muscle is located deep to the long flexor tendons in the adductor-interosseous compartment of the palm. The adductor pollicis is formed by oblique and transverse heads (G11 6.73; Table 6.9 [p. 545];G12 6.70, 6.66D, 6.76D; N450, 453). The former arises from the capitate and the bases of the second and third metacarpal bones, and the transverse head passes laterally from the shaft of the third metacarpal to join it. The adductor pollicis inserts on the medial side of the proximal phalanx of the thumb.
32. To study the deepest structures of the palm reflect the flexor digitorum superficialis and flexor digitorum profundus tendons IN ONE UPPER EXTREMITY ONLY. Cut the flexor digitorum superficialis and profundus tendons just proximal to the wrist and reflect them distally to the bases of the fingers. Leave the superficial palmar arch and common palmar digital nerves intact. In the other hand spread the intact flexor superficialis and profundus tendons as far apart as possible to study deeper structures. Clean the transverse and oblique heads of the adductor pollicis muscle (G11 6.73; G12 6.70). XXX
The deep palmar arch is formed mainly by the radial artery with usually a contribution medially from the deep branch of the ulnar artery (G11 6.73, 6.75; Table 6.10 [p. 553]; G12 6.70, 6.72A-B, Table 6.12 [p. 573]; N453A-B-C, 454A-B). The radial artery enters the palm by piercing the first dorsal interosseous muscle and gives off radialis indicis and princeps pollicis branches. The radialis indicis artery passes along the lateral side of the index finger to supply it. The princeps pollicis artery divides at the base of the proximal phalanx of the thumb into palmar digital branches to supply the sides of the thumb. The radial artery continues between the two heads of the adductor pollicis as the deep palmar arch. Palmar metacarpal arteries branch from the deep palmar arch. They give perforating branches to dorsal metacarpal arteries before ending in the common palmar digital branches of the superficial arch.
The deep branch of the ulnar nerve branches from the ulnar nerve in Guyon’s canal (G11 6.70, 6.73, 6.74; G126.67B, 6.70, 6.71; N448A-B, 453A-B-C, 464). In addition to innervating the hypothenar muscles, the deep branch supplies the medial two lumbrical muscles, all of the interosseous muscles, and the adductor pollicis. The deep branch of the ulnar nerve also supplies the deep head of the flexor pollicis brevis muscle when it is present, while the superficial head of the flexor is typically innervated by the recurrent branch of the median nerve.
33. Cut the oblique head of the adductor pollicis [R430.6] from its origin and reflect it toward the thumb (G11 6.73, 6.75, Table 6.10 [p. 553]; G12 6.70, 6.72A-B, Table 6.12 [p. 573]; N453A-C). The radial artery emerges between the two heads of the adductor as the deep palmar arch [R430.23]. Find and clean the deep branch of the ulnar nerve running parallel to the deep palmar arch. XXX
The dorsal and palmar interosseous muscles are located in the spaces between the metacarpal bones (G11 6.74, 6.79; Table 6.9 [p. 545]; G12 6.71, 6.76, 6.66D, 6.76D; N452A-B-C, 453A-B-C, 458A-B). There are four dorsal interossei but only three palmar interossei because the palmar interosseous muscle between the first and second metacarpals fuses with the adductor pollicis during development. Dorsal interossei attach into both the proximal phalanges and extensor expansions on the lateral sides of digits two and three and the medial side of digits three and four. The palmar interossei insert on the medial side of digit two and the lateral sides of digits four and five. These attachments make it easy to remember the functions of the interossei: the dorsal interossei abduct digits (easily remembered as “dab”) from the reference digit of the hand (middle finger), and the palmar interossei adduct digits (pad). Both groups of interosseous muscles also assist with MP flexion when combined with PIP and DIP extension.
34. Try to identify palmar and dorsal interosseous muscles. Although only the dorsal interossei can be seen on the dorsum of the hand, from the palmar side both dorsal and palmar interossei are visible, and the easiest way to distinguish them is by their distal attachments. In one hand make a short incision between the heads of metacarpal bones four and five and spread them slightly apart to study the insertions of the adjacent dorsal and palmar interossei. The dorsal interosseous muscle [R394.10] will have an insertion on the medial side of the proximal phalanx of digit four and the palmar interosseous [R394.5] will have an insertion on the lateral side of digit five.
POSTERIOR FOREARM
35. Turn your attention to the posterior (extensor) compartment of the forearm. The cadaver may have to be repositioned to perform this dissection. If the skin has not been completely removed from the forearm, do so now. Also remove the thin skin from the dorsum of the hand at this time. Make an incision through the skin straight down the back of the hand to the tip of the third finger (Fig. 6-1). Then make a transverse incision across the dorsum just proximal to the heads of the metacarpals (knuckles). Remove the skin.

36. Find the cephalic and basilic veins, which begin in the dorsal venous arch of the hand (G11 6.6B & E; G12 6.10B & E; N404A-B). Note the posterior antebrachial cutaneous nerve [R416.3] in the distal forearm, a branch of the radial nerve, but don’t spend a lot of time cleaning it (G11 6.4B, 6.78; G12 6.6B, 6.75A-B-C; N404A-B). Remember that the lateraland medial antebrachial cutaneous nerves supply the lateral and medial borders, respectively, of the posterior forearm. Knowledge of the distributions of these cutaneous nerves is clinically useful, but we don’t have time to dissect them.
37. Remove the antebrachial fascia [R416.2] over the extensor compartment. Similar to the antebrachial fascia over the flexor compartment, it is adherent to the underlying muscle fibers, which take part of their origin from it. Preserve the extensor retinaculum [R417.11] on one upper extremity. It is a transverse thickening of antebrachial fascia connecting the distal ends of the radius and ulna (G11 6.76, 6.77; G12 6.73A-B-C-D, 6.74A-B; N432, 457, 458A-B ). The extensor retinaculum prevents bowstringing of the tendons during wrist extension. XXX
The muscles of the posterior compartment of the forearm are divided into superficial and deep layers. Four of the superficial group of forearm extensor muscles share a proximal attachment (common extensor tendon) from the lateral epicondyle of the humerus, and the other two superficial muscles attach to the lateral supracondylar ridge. The superficial group consists of, from lateral to medial, the brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris (G11 6.76A; G12 6.73A; N432).
The brachioradialis muscle passes from the upper 2/3 of the lateral supraconylar ridge of the humerus to the lateral surface of the radius just proximal to the styloid process (G11 6.60, 6.62, 6.76, 6.77, Table 6.11 [p. 555]; G12 6.57B, 6.59B, 6.73A-B-C-D, 6.74A-B, Table 6.13 (1-2), (3-4) [p. 575]; N432, 433, 334, 435, 438). It is the only muscle in the superficial group of forearm extensors that doesn’t cross the wrist joint. The brachioradialis is an unusual muscle in that it is innervated by the radial nerve but helps to flex the forearm when additional speed or force is required. It may perform weak elbow flexion in a patient who has a lesion of the musculocutaneous nerve, which would paralyze the brachialis and biceps brachii.
The extensor carpi radialis longus takes origin from the lower 1/3 of the lateral supracondylar ridge of the humerus and attaches distally to the base of the second metacarpal bone (G11 6.76A & C, 6.77A; G12 6.73A & C, 6.74A; N429A-B, 432, 433).
The extensor carpi radialis brevis passes from the common extensor tendon on the lateral epicondyle to the base of the third metacarpal. The humeral attachment of this muscle becomes inflamed due to repeated forceful wrist extension in lateral epicondylitis (tennis elbow). The two extensor carpi radialis muscles extend the hand at the wrist joint and abduct (radially deviate) it.
The extensor digitorum divides into tendons for digits 2-5 proximal to the extensor retinaculum. Note that the extensor digitorum tendon for the little finger may not separate from that of the ring finger until near the heads of the metacarpal bones. The tendons will be followed into the hand later, where they form an extensor expansion over the proximal phalanx of each digit (G11 6.79B & D, 6.80; G12 6.76B & E, 6.77; N429A-B, 452A-B-C, 458A-B). The extensor digitorum extends digits 2-5 during gross opening and closing movements of the hand and can help to extend the wrist.
The extensor digiti minimi lies medial to the extensor digitorum. It goes to the little finger (digit 5), usually receiving a tendinous band from the extensor digitorum tendon of the ring finger just proximal to the MP joint (G11 6.79B & D; G12 6.76B & E; N429A-B, 432, 458A-B). The tendon of extensor digiti minimi itself frequently divides into two tendons before entering the little finger (G11 6.79B & D; G12 6.76B & E; N458A-B). The extensor digiti minimi provides independent extension of the little finger.
The most medial muscle in the superficial group is the extensor carpi ulnaris muscle, which passes from the common extensor tendon to the base of the fifth metacarpal bone. It extends and adducts (ulnarly deviates) the hand at the wrist. During routine extension of the hand at the wrist, the extensor carpi ulnaris and the two extensor carpi radialis muscles are the prime movers.
38. Clean the superficial group of forearm extensor muscles. Separate the brachioradialis [R390.13] and the extensor carpi radialis longus [R390.14]. Both take origin from the lateral supracondylar ridge of the humerus. Verify that the brachioradialis attaches distally on the radius just proximal to the wrist (radiocarpal) joint. It is unusual among the posterior forearm muscles both in that it flexes the elbow and in that it cannot produce wrist movements.
39. The extensor carpi radialis longus is overlapped by the brachioradialis and in turn partially covers the shorter and deeper extensor carpi radialis brevis [R390.15], which shares an origin from the lateral epicondyle with the remaining superficial extensor muscles. The tendons of the extensor carpi radialis longus and brevis course deep to the tendons of forearm extensor muscles to the thumb—abductor pollicis longus [R390.16], extensor pollicis brevis [R390.17], and extensor pollicis longus [R390.18]—near the wrist. The extensor carpi radialis longus and brevis muscles’ insertions on the base of the second and third metacarpal bones, respectively, may be difficult to see at this time.
40. Clean the extensor digitorum muscle [R390.7]. Find its tendons in the distal forearm as they approach the extensor retinaculum [R390.9]. The termination of the tendons in digits 2-5 will be seen during dissection of the hand. Identify the extensor digiti minimi [R390.10] medial to the extensor digitorum. Note that the extensor digiti minimi tendon often splits into two before entering the dorsum of the little finger. The extensor digiti minimi is often considered a subdivision of the extensor digitorum but provides independent extension of the little finger.
41. Clean the most medial of the superficial forearm extensor muscles, the extensor carpi ulnaris [R390.6]. The insertion of its tendon on the base of the fifth metacarpal bone is just distal to the extensor retinaculum. XXX
The deep group of forearm extensor muscles consists of the supinator, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis muscles. The supinator muscle passes from the lateral epicondyle of the humerus, radial collateral and anular ligaments, and supinator crest and fossa of the ulna to the lateral and posterior surfaces of the proximal 1/3 of the radius (G11 6.61A-B-C, 6.63, 6.77; G12 6.58B, 6.60B, 6.74A-B; N428A-B, 438). The deep branch of the radial nerve pierces the supinator muscle and emerges into the posterior compartment of the forearm with a new name, the posterior interosseous nerve (G11 6.77; G12 6.74A-B; N433). The supinator is always active in supination of the forearm but is assisted by the biceps brachii during rapid supination or against resistance.
The deep branch of the radial nerve may become entrapped within the supinator muscle or damaged by a fracture of the neck of the radius. Since the branches to the extensor carpi radialis muscles arise more proximally, wrist extension is spared but there is loss of thumb extension and MP extension of fingers 2-5. In this lesion, how is interphalangeal extension of digits 2-5 still possible when it is combined with MP flexion?
The abductor pollicis longus attaches proximally to the radius, ulna, and interosseous membrane. From this origin it passes distally to attach on the base of the first metacarpal bone (G11 6.76A, 6.77; G12 6.73A, 6.74A-B; N429A-B, 433, 439). The abductor pollicis longus abducts and extends the carpometacarpal (CM) joint of the thumb. Traveling with the abductor pollicis longus, and sometimes partially fused with it, is the extensor pollicis brevis. This muscle traverses the forearm from a proximal attachment on the radius and interosseous membrane to the base of the proximal phalanx of the thumb. The extensor pollicis brevis extends the metacarpophalangeal (MP) joint of the thumb. Observe the relationship of these two muscles in your cadaver.
The tendons of abductor pollicis longus and extensor pollicis brevis share a tendon sheath and compartment deep to the extensor retinaculum (G11 6.79B-C; G12 6.76B-C; N433, 458A-B). They may become inflamed deep to the retinaculum following repetitive movements (de Quervain’s stenosing tenosynovitis, de Quervain’s syndrome), causing tenderness and lateral wrist pain that may radiate both proximally and distally. The differential diagnosis includes arthritis of the first carpometacarpal joint and scaphoid fracture.
Identify the extensor pollicis longus muscle, which passes from the middle 1/3 of the ulna and interosseous membrane to the distal phalanx of the thumb. It extends the distal phalanx of the thumb at the interphalangeal (IP) joint and can help extend the MP joint.
The tendon of extensor pollicis longus forms the posterior boundary of a depression visible when the thumb is fully extended, the anatomical snuffbox (G11 6.76A & D, 6.77A, 6.81B-D; G12 6.73A & D, 6.74A, 6.78B-D; N432, 455, 457). The anterior boundary is the tendons of abductor pollicis longus and extensor pollicis brevis. The pulse of the radial artery can be felt in the anatomical snuffbox, which it traverses. The floor of the snuffbox is formed by the radial styloid process, scaphoid, and trapezium bones.
The scaphoid is the most frequently fractured carpal bone. Pain with hand movement and tenderness on deep palpation in the anatomical snuffbox following a fall on an outstretched hand are characteristic of a scaphoid fracture. The fracture itself may not be apparent on x-rays for 10-14 days, until bone resorption has occurred at the fracture site. A scaphoid fracture may result in interruption of the blood supply with avascular necrosis of the proximal fragment.
The extensor indicis has a proximal attachment from the distal 1/3 of the ulna and interosseous membrane (G11 6.77; G12 6.74A-B; N429A-B, 433). Look for the tendon of this muscle, which will attach into the extensor expansion of the index finger. The extensor indicis provides extension of the index finger independent of the extensor digitorum muscle.
42. Bluntly separate the bracioradialis from the brachialis muscle in the distal arm. Retract the brachioradialis laterally to expose radial nerve. Follow the radial nerve distally to where it branches into superficial and deep branches. Clean the supinator muscle [R417.27] and identify the deep branch of the radial nerve [R393.5] entering it (G11 6.62, 6.63; G12 6.59B, 6.60B; N435). You may have to retract the extensor carpi radialis muscles to do so.
43. In the middle of the posterior side of the forearm spread apart, but do not cut, the superficial group of extensor muscles in order to expose the deep group. Find the continuation of the deep branch of the radial nerve emerging from the supinator, where it is now called the posterior interosseous nerve [R417.24]. Note that the posterior interosseous nerve runs in the fascial plane between the superficial and deep forearm extensor muscles (G11 6.77; G12 6.74A-B; N433, 466A-B) instead of on the surface of the interosseous membrane as the anterior interosseous nerve does.
44. Distal to the supinator find the abductor pollicis longus [R417.19] and extensor pollicis brevis [R417.21] muscles taking origin adjacent to each other (G11 6.77; G12 6.74A-B; N433). Follow the tendon of the abductor pollicis longus to the extensor retinaculum. The insertion of the tendon on the base of the first metacarpal bone may be difficult to see at present. The tendon of the extensor pollicis brevis runs adjacent to that of the abductor and shares a synovial sheath with it. The extensor pollicis brevis tendon attaches on the proximal phalanx of the thumb.
45. The extensor pollicis longus [R417.8] is located medial to the other two pollicis muscles. Its tendon passes almost vertically downward and then hooks around the dorsal tubercle of the radius, using it as a pulley, to angle laterally to the thumb. The extensor pollicis longus tendon forms the posterior boundary of the anatomical snuffbox [R394.11]. Identify the radial artery [R417.23] within the snuffbox. Later, when your hands are clean, extend your thumb and find your own anatomical snuffbox. Palpate deeply within it to find the pulse of the radial artery.
46. Identify the extensor indicis [R417.9] and trace its tendon as far distally as the extensor retinaculum. The extensor indicis tendon joins the extensor expansion of the index finger to provide independent extension of the digit. XXX
The radial nerve divides into superficial and deep branches anterior to the lateral epicondyle in the fascial interval between the brachioradialis and brachialis muscles (G11 6.49D, 6.62; G12 6.45D, 6.59B; N435). The superficial branch of the radial nerve (superficial radial nerve), a cutaneous nerve that descends under cover of the brachioradialis to the distal forearm, passes laterally superficial to the anatomical snuffbox to reach the dorsum of the hand (G11 6.60, 6.78, 6.81A; G12 6.57B, 6.75A-B-C, 6.78A; N404A-B, 435, 455). It provides cutaneous innervation to the dorsum of the hand and lateral 3½ digits, except over the distal phalanges, where the skin is supplied by branches of the median nerve.
The deep branch of the radial nerve (deep radial nerve) pierces the supinator muscle and emerges between the superficial and deep groups of forearm extensor muscles as the posterior interosseous nerve (G11 6.77A; G12 6.74A; N433, 466A-B). It courses distally in the fascial plane between the superficial and deep muscles. In summary, the radial nerve typically sends branches to innervate the brachioradialis and extensor carpi radialis longus before dividing into superficial and deep branches. The deep branch of the radial nerve usually supplies the extensor carpi radialis brevis and supinator muscles before piercing the latter, and the posterior interosseous nerve supplies the remaining forearm extensor muscles. Therefore, injury to the deep branch of the radial nerve at the supinator muscle spares wrist extension.47. Observe that the radial nerve divides into its superficial and deep branches anterior to the lateral epicondyle in the fascial interval between the brachioradialis [R421.3] and brachialis [R421.2] (G11 6.49, 6.62; G12 6.45D, 6.59B; N435). Follow the superficial radial nerve [R421.4], a cutaneous nerve that descends under cover of the brachioradialis to the distal forearm, where it passes laterally superficial to the anatomical snuffbox to reach the dorsum of the hand (G11 6.60, 6.78, 6.81A; G12 6.57B, 6.75A-B-C, 6.78A; N435, 455, 466A-B). Again trace the deep radial nerve [R421.5] into the supinator muscle and find where it emerges as the posterior interosseus nerve [R417.24]. XXX
After passing above the upper border of the interosseous membrane to enter the posterior compartment of the forearm, the posterior interosseous artery gives off the interosseous recurrent artery and descends with the posterior interosseous nerve between the superficial and deep layers of forearm extensor muscles (G11 6.77A; G12 6.74A; N422, 433). Just above the wrist the anterior interosseous artery pierces the interosseous membrane to enter the posterior compartment en route to the dorsal carpal arch (G11 6.11D, 6.58B; Table 6.10 [p. 553]; G12 6.7D, 6.55C, Table 6.12 [p. 573]; N433, 457). Therefore, the anterior interosseous artery substitutes distally for the short posterior interosseous artery.
48. Locate the posterior interosseous artery between the superficial and deep layers of forearm extensor muscles and note whether or not the posterior interosseous nerve runs with it. Near the wrist spread the extensor tendons apart to find the anterior interosseous artery piercing the interosseous membrane from the anterior compartment. XXX
The extensor retinaculum is a transverse thickening of antebrachial fascia. It has an attachment to the distal radius laterally and to the distal ulna and triquetrum medially (G11 6.76A, 6.77A; G12 6.73A, 6.74A; N432, 458A-B). The space deep to the extensor retinaculum is subdivided into six osseofibrous compartments by connective tissue septa (G11 6.79B-C; G12 6.76B-C; N458A-B). Note the contents of each compartment. The most lateral compartment contains the tendons of abductor pollicis longus and extensor pollicis brevis. The second compartment, which includes the anatomical snuffbox, contains the tendons of extensor carpi radialis longus and brevis. The third compartment has only one tendon traversing it, the extensor pollicis longus tendon. The broad fourth compartment over the middle of the dorsum of the distal forearm contains the tendons of extensor digitorum and the deeper extensor indicis. The extensor digiti minimi tendon occupies the fifth compartment. The final, most medial, compartment contains the tendon of extensor carpi ulnaris.
DORSUM OF THE HAND
49. Again find the dorsal venous arch [R398.13] that gives rise to the cephalic and basilic veins (G11 6.6B & E; G12 6.10B & E; N404A-B, 456). Be aware of the distribution of the cutaneous nerves on the dorsum of the hand (G11 6.4B, 6.78; G12 6.6B, 6.75A-B-C; N402A-B, 404A-B). The dorsal cutaneous branch of the ulnar nerve [R417.12]supplies the dorsal surface of the medial hand and medial 1½ digits, except over the distal phalanges, which are supplied by proper palmar digital branches of the ulnar nerve. The superficial radial nerve [R417.22] supplies the lateral half of the dorsum of the hand and the lateral 3½ digits, except over the distal phalanges, where the skin and nail beds are supplied by proper palmar digital branches of the median nerve.
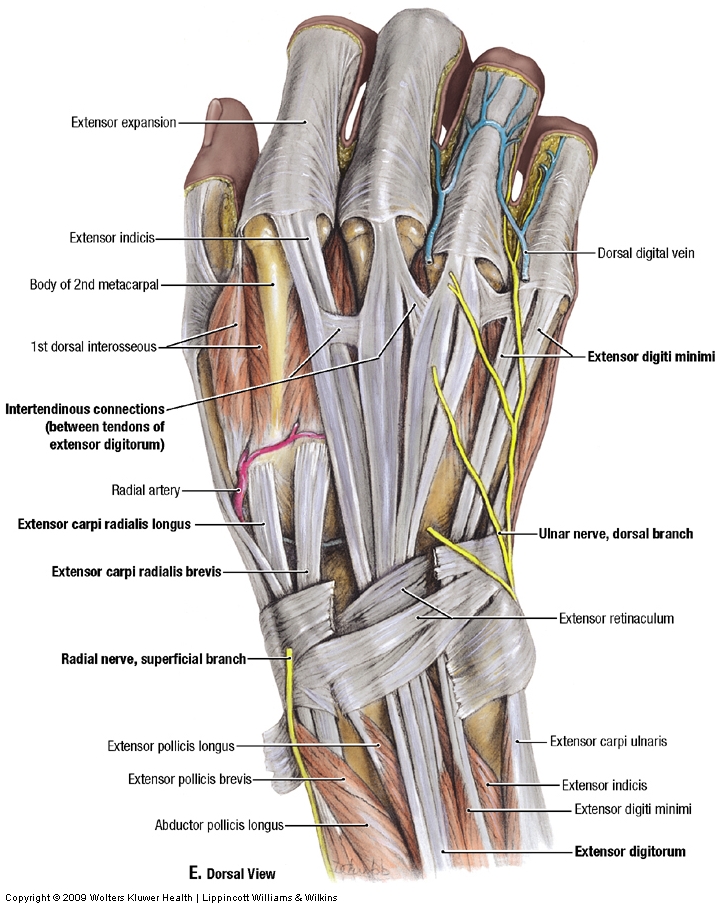
50. Find intertendinous connections between the tendons of the extensor digitorum (G11 6.79B & D; G12 6.76B & E; N429A-B, 458A-B). These connections limit independent extension of the middle and ring fingers (e.g., make a fist and then try to extend only your ring finger). While preserving the tendons of the forearm extensor muscles, dissect deep to them to study the arteries on the dorsum of the hand. Briefly attempt to find the dorsal carpal arch formed by dorsal carpal branches of the radial and ulnar arteries, with usually a contribution from the anterior interosseous artery (G11 6.76A & D, Table 6.10 [p. 553]; G12 6.73A & D, Table 6.12 [p. 573]; N 457). The dorsal carpal arch has dorsal metacarpal arteriesbranching from it, which divide into dorsal digital arteries. Don’t spend a lot of time dissecting them. Follow the radial artery through the anatomical snuffbox to where it pierces the first dorsal interosseous muscle to enter the palm of the hand (G11 6.76A, 6.77A; G12 6.73A, 6.74A; N 455, 457).
51. Clean one or more of the four dorsal interosseous muscles [R391.9] and note their bipennate structure (i.e., they have a central tendon with muscle fibers converging on it from each side in a feather-like arrangement). The dorsal interossei insert on the lateral sides of digits two and three and the medial sides of digits three and four (G11 6.79B, Table 6.9 [p. 545]; G12 6.76B, 6.66D, 6.76D; N 453A-B-C). The dorsal interossei abduct digits from the reference digit of the hand (middle finger) and assist with MP flexion when it is combined with PIP and DIP extension.
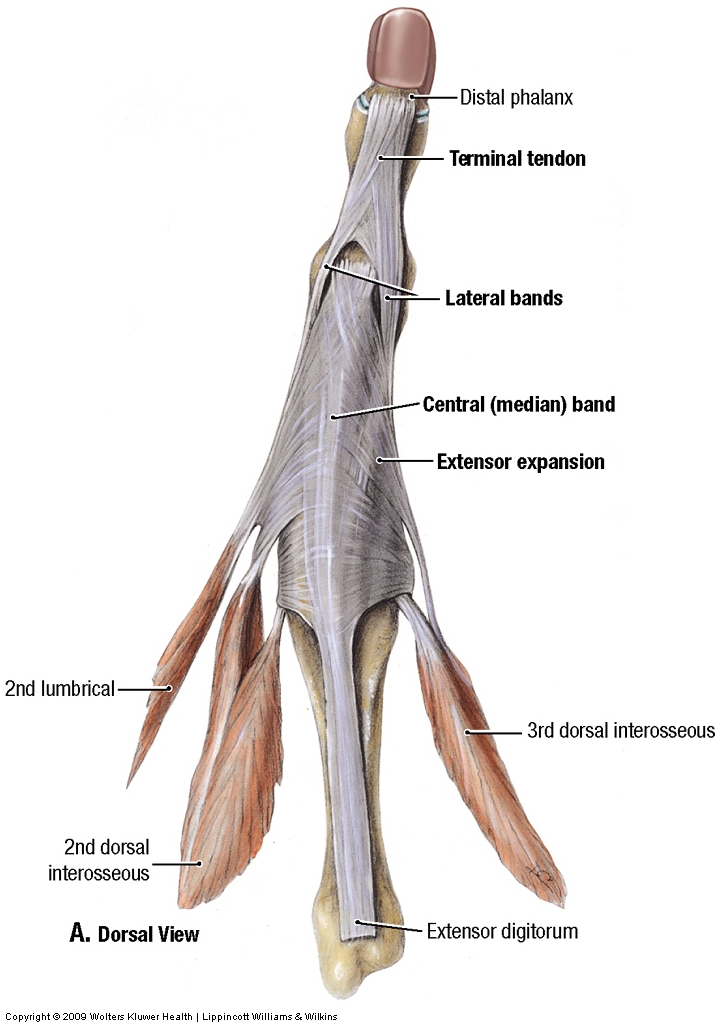
52. On the third finger and at least one other digit clean an extensor expansion (extensor hood) formed by the tendon of the extensor digitorum muscle (G11 6.79D, 6.80; G12 6.76E, 6.77; N452A-B-C, 458A-B). Each tendon divides into a central band that attaches to the middle phalanx and two lateral bands that attach to the distal phalanx. The interosseous and lumbrical muscles have insertions into the extensor expansions (G11 6.80A-B; G12 6.77A-B; N452A-B-C). XXX
{kind=link}
{kind=link}
The illustrations in this dissection guide are used with permission from Gray’s Anatomy for Students. 2005, by Richard Drake, Wayne Vogel, and Adam Mitchell, Elsevier Inc., Philadelphia; and from Grant’s Atlas of Anatomy, 11E, 2005, Anne Agur and Arthur Dalley II, Lippincott Williams & Wilkins, Philadelphia.