Foot and Ankle
The foot is the part of the lower extremity distal to the ankle. It is a base for supporting the body when standing, and downward movement of the foot at the ankle (plantar flexion) provides part of the physical force for locomotion. The part of the foot that contacts the ground or floor is the sole or plantar region, and the part that faces superiorly is the dorsum or dorsal region.
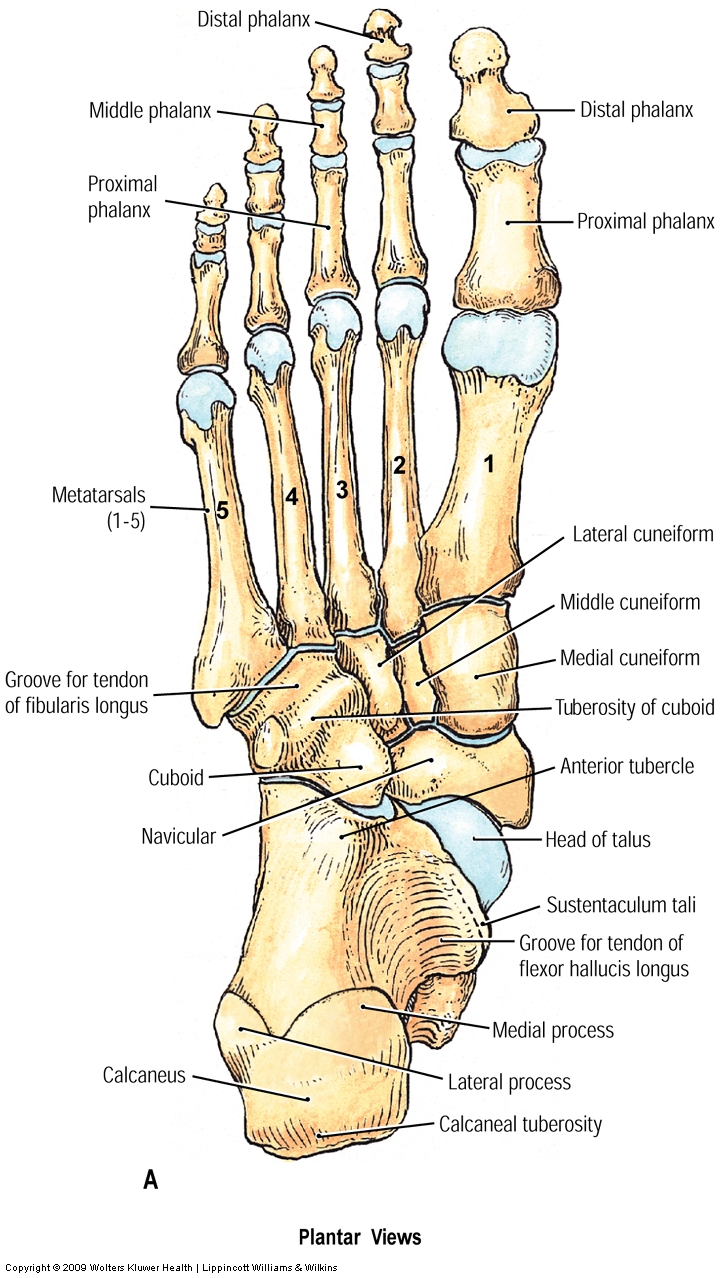
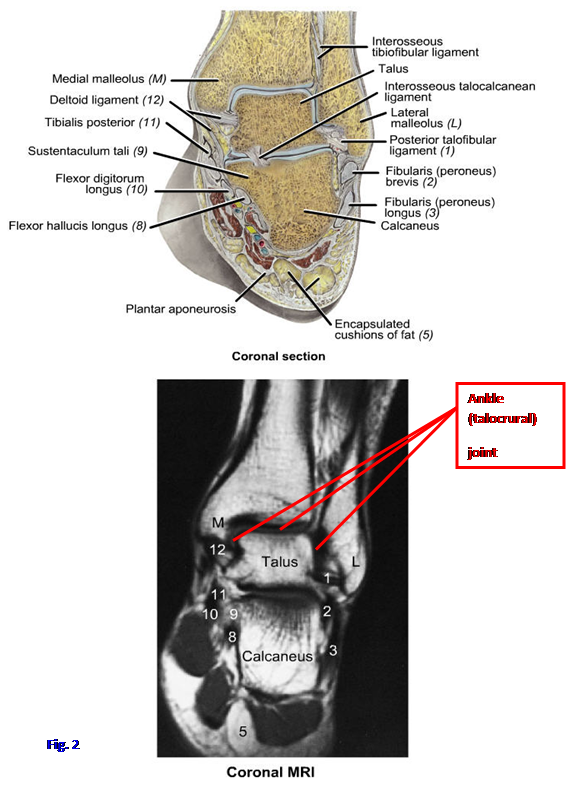
The skeleton of the foot is formed by 7 tarsal bones, 5 metatarsal bones, and 14 phalanges (Fig. 1; Gr 5.68; Tables 5.13 [p. 429], 5.15 [p. 431]; Ne 511, 512). The tarsal bones are the talus, calcaneus, navicular, three cuneiform bones, and the cuboid. The talus consists of a head, neck, and body. The body of the talus has a superior part (trochlea) that articulates with the tibia and fibula at the ankle (talocrural) joint (Fig. 2; Gr 5.73; Ne 512). The anterior part of the trochlea is wider than the posterior part so that the ankle joint is more stable when the foot is rotated upward toward the leg (dorsiflexion) than downward toward the floor (plantar flexion). Therefore, ankle sprains are more likely to occur in the plantarflexed position. The posterior articular facet on the inferior surface of the body of the talus forms the subtalar joint with the calcaneus (Gr 5.77B). The subtalar joint is important in turning the sole of the foot inward toward the median plane (inversion) and outward away from the median plane (eversion), allowing the foot to accommodate to uneven ground.
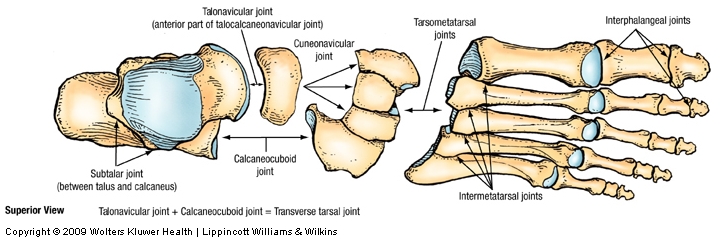
The head of the talus articulates anteriorly with the navicular bone at the talonavicular (talocalcaneonavicular) joint, which is the medial part of the transverse tarsal joint (Fig. 1; Gr 5.78; Table 5.16 [p. 442]; Ne 511, 512). The transverse tarsal joint functions in inversion and eversion, as well as adduction and abduction of the anterior part of the foot on the hindfoot. The head of the talus is joined to its body by the neck of the talus. The neck of the talus may be fractured in a severe dorsiflexion injury (e.g., during an automobile collision when the driver has his foot pressed firmly against the brake pedal at the moment of impact). A fracture of the talar neck is significant because the main blood supply enters the body of the talus from anteriorly, through the neck, and a fracture that interrupts it may result in avascular necrosis of the body of the talus.
The large calcaneus is the heel bone (Fig. 1; Gr 5.68; Ne 511, 512, 513). On the inferior aspect of the calcaneus, the tuberosity is the posterior, weight-bearing portion that transmits 50% of the weight supported on that foot to the ground. The posterior end of the calcaneus receives the attachment of the calcaneal (Achilles) tendon, allowing the gastrocnemius and soleus to strongly plantar flex the foot.
The superior surface of the calcaneus has three large articular facets. The middle third of the superior surface carries the posterior articular facet, which articulates with the talus at the subtalar joint (Gr 5.81; Table 5.16 [p. 442]; Ne 512, 513). Middle and anterior articular facets on the calcaneus articulate with corresponding facets on the talus in the talocalcaneonavicular joint, which is actually two joints sharing a single synovial cavity (Gr 5.77B). Medially the calcaneus has a horizontal shelf, the sustentaculum tali, which bears the middle facet and helps to support the talus (Gr 5.68A & D-E; Ne 511, 512, 513). The calcaneus articulates anteriorly with the cuboid. The latter articulation, the calcaneocuboid joint, forms the lateral part of the transverse tarsal joint (Fig. 1; Gr Table 5.16 [p. 442]; Ne 511, 512).
{kind=link}
{kind=link}
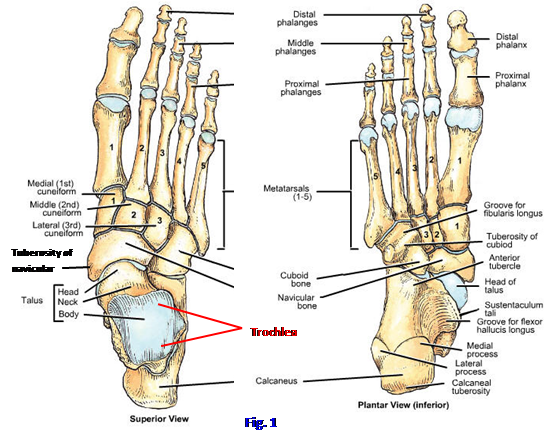
The navicular bone is interposed between the head of the talus posteriorly and the three cuneiform bones anteriorly (Fig. 1; Gr 5.68D-E, 5.82; Ne 511, 512). It articulates with these four bones and laterally with the cuboid bone. The most prominent feature of the navicular is the navicular tuberosity. It provides attachment for the tibialis posterior tendon. If it is too large, the navicular tuberosity may press against a shoe to produce foot pain.
The three cuneiform bones are the medial (1st), intermediate (2nd), and lateral (3rd) cuneiforms. They articulate proximally with the navicular bone and each forms a tarsometatarsal joint with the corresponding member of the first three metatarsal bones. The lateral cuneiform also articulates laterally with the cuboid bone.
The cuboid is the tarsal bone located lateral to the navicular and lateral cuneiform bones, between the calcaneus proximally and the fourth and fifth metatarsal bones distally (Fig. 1). Its most notable features are present on its plantar (inferior) surface. An almost transverse ridge on the plantar surface is the tuberosity of the cuboid, which is located just behind the groove for the tendon of the fibularis longus muscle (Gr 5.68A, 5.82; Ne 511, 512).
The five metatarsal bones of the foot correspond to the metacarpal bones of the hand but are more substantial (Fig. 1; Gr 5.68; Ne 511, 512). They articulate proximally at tarsometatarsal joints and distally at metatarsophalangeal (MP) joints (Gr Table 5.16 [p. 442]). Each metatarsal bone consists of a proximal base, intermediate shaft (body), and distal head. The metatarsals are numbered 1 to 5 from the medial (great toe) side. The first metatarsal is shorter and thicker than the more lateral metatarsal bones because its head bears twice as much weight. The second metatarsal is the longest, and its base fits into a recess formed because the intermediate cuneiform bone is shorter than the medial and lateral cuneiforms (Gr 5.68A; Ne 511). The fifth metatarsal bone has a prominent lateral tuberosity on its base for attachment of the fibularis brevis tendon. The tuberosity of the fifth metatarsal may be avulsed by the fibularis brevis during forced inversion of the foot.
The great toe has only proximal and distal phalanges (Fig. 1; Gr 5.68A; Ne 511). Toes 2-5 have proximal, middle, and distal phalanges. Like the larger metatarsal bones, the phalanges are miniature long bones with a base, shaft, and head. The proximal interphalangeal (PIP) joint is formed between the proximal and middle phalanges of toes 2-5, and the distal interphalangeal (DIP) joint is formed between the middle and distal phalanges. Since there are only two phalanges in the great toe, there is only one interphalangeal joint.
1. Examine the bones of the foot on an intact skeleton and on x-rays. Find the head, neck, and body of the talus. At the ankle joint note that the body of the talus forms a superior tenon (projection) that fits into a mortise (slot or recess) formed by the medial and lateral malleoli and the distal end of the tibial shaft (Fig. 2). Verify that the superior part of the talus, or trochlea, is wider anteriorly than posteriorly (Fig. 1).
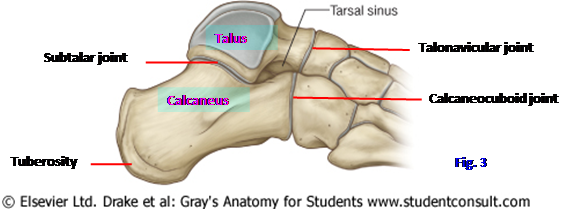
2. The head of the talus articulates anteriorly with the navicular bone at the talonavicular (talocalcaneonavicular) joint, which is the medial part of the transverse tarsal joint. Identify the talonavicular joint and the lateral part of the transverse tarsal joint, the calcaneocuboid joint (Fig. 3).
3. Find the prominent tuberosity of the calcaneus, which transfers weight to the ground. On the medial side of the calcaneus study the horizontal sustentaculum tali, which helps to support the talus and gives attachment to the important plantar calcaneonavicular (spring) ligament. On the lateral side look for a small projection, the fibular trochlea, which may be present. Superiorly the calcaneus articulates with the talus at the subtalar joint. Look at the talus and calcaneus from the lateral side. Identify a gap, the tarsal sinus, which is apparent on radiographs anterior to the subtalar joint, between it and the anterior articulations of the two bones at the talocalcaneonavicular joint (Fig. 3; Gr 5.80B; Ne 512, 514 [not labeled]). The tarsal sinus is occupied in life by the interosseous talocalcaneal ligament.
4. Note the tuberosity on the medial side of the navicular bone (Fig. 1). The tuberosity is easily palpable on your own foot. Identify the medial, intermediate, and lateral cuneiform bones distal to the navicular bone. Each articulates proximally with the navicular bone and distally with a metatarsal bone at a tarsometatarsal joint. The lateral cuneiform also articulates with the cuboid bone laterally.
5. Turn your attention to the cuboid bone. Proximally it articulates with the calcaneus at the calcaneocuboid joint. Medially it articulates with the navicular and lateral cuneiform bones. Distally the cuboid forms tarsometatarsal joints with the fourth and fifth metatarsals. On its plantar surface identify the tuberosity of the cuboid bone posterior to the groove for the fibularis longus tendon.
6. The metatarsal bones are numbered 1-5 from the side of the great toe. Each has a proximal base, intermediate shaft, and distal head. Note in the articulated foot that the heads of the metatarsal bones are the part that makes contact with the floor.
7. The great toe has proximal and distal phalanges articulating at an interphalangeal joint. The other four digits have a middle phalanx between the proximal and distal phalanges and, therefore, have proximal (PIP) and distal (DIP) interphalangeal joints. Verify this. XXX
The normal foot is not a flat structure, but rather has arches that give it flexibility to adapt to uneven ground surfaces and to provide shock absorption. The arches also function in distributing the weight transferred to the foot from the leg so that normally weight is transmitted to the ground only at the tuberosity of the calcaneus (50%) and the heads of the metatarsal bones (50%) (Gr 5.66C, 5.68C, D, E; Ne 512).
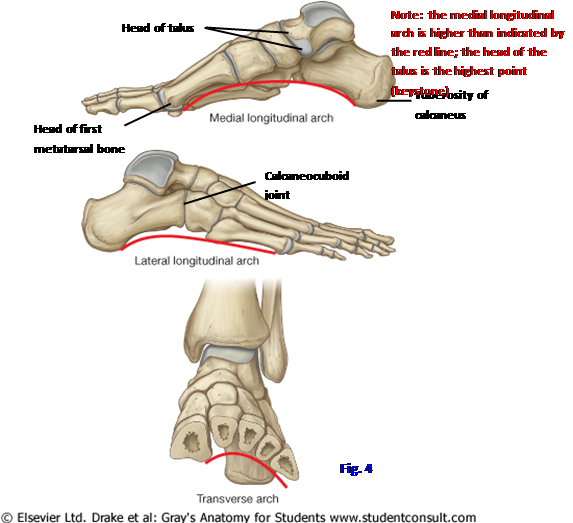
The tarsal and metatarsal bones are arranged into longitudinal and transverse arches (Fig. 4; Gr 5.68C, D, E; Ne 512). The longitudinal arch of the foot may be subdivided into a medial longitudinal arch and a lateral longitudinal arch. The medial longitudinal arch is higher than the lateral longitudinal arch and is formed by the calcaneus, talus, navicular, three cuneiform bones, and the first three metatarsal bones (Figs. 1, 4). The head of the talus is the highest point (keystone) of the medial longitudinal arch. The head of the talus rests upon the plantar calcaneonavicular ligament, often called the “spring ligament,” which is especially important in supporting the medial longitudinal arch (Gr 5.82, 5.83; Ne 515, 516). This ligament passes from a posterior attachment on the sustentaculum tali to the navicular bone.
The lateral longitudinal arch is made up of the calcaneus, cuboid, and lateral two metatarsal bones (Figs. 1, 4; Gr 5.68A, C; Ne 512). It is flatter than the medial longitudinal arch and rests on the ground during standing, as reflected by the lateral side of the foot making an impression as part of a normal footprint. The calcaneocuboid joint is the highest point of the lateral longitudinal arch. The chief support of the lateral longitudinal arch is by the long plantar and plantar calcaneocuboid (short plantar) ligaments (Gr 5.82, 5.83; Ne 515, 516). The long plantar ligament attaches posteriorly to the calcaneus and anteriorly to the tuberosity of the cuboid bone and bases of the metatarsals. The plantar calcaneocuboid ligament lies deep to, and partially hidden by, the long plantar ligament. It attaches posteriorly to the anterior tubercle of the calcaneus and anteriorly to the cuboid.
The transverse arch of the foot runs from side to side at the level of the distal row of tarsal bones and bases of the metatarsal bones (Fig. 4). It is formed by the three cuneiform bones, the cuboid bone, and the bases of the metatarsal bones.
The major support of the arches of the foot is still a matter of some debate. Both passive and dynamic factors probably are important. Passive support comes from the general shape of the articulated foot bones, which tend to be somewhat wedge-shaped with the thin part of the bones inferior ( ![]() ). The heavy plantar ligaments—plantar calcaneonavicular, long plantar, and plantar calcaneocuboid ligaments—and interosseous ligaments are important supports (Gr 5.82, 5.83; Ne 516). The plantar aponeurosis also functions as a plantar ligament to contribute support to the arch.
). The heavy plantar ligaments—plantar calcaneonavicular, long plantar, and plantar calcaneocuboid ligaments—and interosseous ligaments are important supports (Gr 5.82, 5.83; Ne 516). The plantar aponeurosis also functions as a plantar ligament to contribute support to the arch.
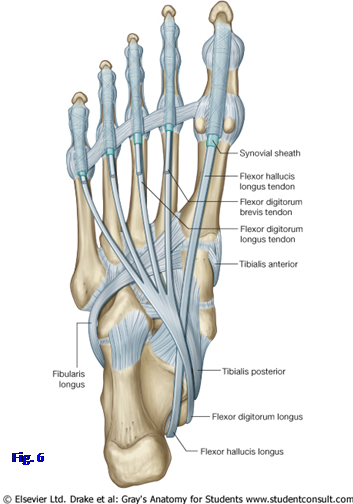
Dynamic support of the arches of the foot is provided by intrinsic muscles of the sole of the foot and long leg muscles with tendons that extend the foot. The muscles of the leg that are most important in supporting the arches are the fibularis longus, tibialis anterior, and tibialis posterior muscles. The fibularis longus tendon crosses the sole of the foot from lateral to medial to insert into the medial cuneiform and base of the first metatarsal bone (Fig. 6; Gr 5.82A, Table 5.15 [p. 431]; Ne 516). The tibialis anterior tendon descends from the anterior compartment of the leg to also insert into the medial cuneiform and base of the first metatarsal (Gr 5.64A-B; Ne 515, 516). Together these two muscles form a sling that probably helps to support the medial longitudinal arch.
The tibialis posterior likewise helps to support the arch (Fig. 6; Gr 5.64A-B). Remember that the tibialis posterior and tibialis anterior muscles are inverters of the foot, and the fibularis longus is an everter. Part of the role of these muscles in supporting the arches of the foot may be to maintain the foot between inversion and eversion to avoid undue strain. Excessive eversion in particular favors downward and forward slipping of the head of the talus with collapse of the medial longitudinal arch.
8. The weight on a lower extremity is transmitted to the ground in a normal foot only on the tuberosity of the calcaneus (50%) and the heads of the metatarsal bones (50%) (Fig 4. [upper and middle]; Gr 5.66C, 5.68C, D, E; Ne 512). The head of the first metatarsal bone bears twice as much weight as that of any of the lateral four metatarsal bones and thus is stouter. Study the longitudinal and transverse arches of the foot in an articulated foot skeleton. Verify that the head of the talus lies at the highest point of the medial longitudinal arch and the calcaneocuboid joint occupies the highest point of the lateral longitudinal arch. Note that the transverse arch is obvious only at the level of the distal tarsal bones. XXX
The foot of the toddler normally appears flat due to hypermobile joints and a thick subcutaneous fat pad in the sole. After about the age of three, fat is lost and the medial longitudinal arch starts to become visible. The lax ligaments of the infant become stronger and the hypermobile joints become more stable spontaneously with age, so that an arch develops. If an arch isn’t present in the foot of an adolescent or adult, the patient is said to have flatfeet (pes planus). Flatfeet can be either flexible or rigid. Flexible flatfeet appear flat when weight-bearing but have an arch when not weight-bearing (e.g., sitting with the feet hanging over the side of the examination table). The condition may or may not be symptomatic.
Rigid flatfeet are flat even when the patient is non-weight-bearing and are symptomatic. They are usually painful and may be associated with spasm and contracture of the fibularis muscles. Rigid flatfeet may be congenital or acquired. The congenital form usually results from bone deformities, including the fusion of adjacent tarsal bones (tarsal coalition), typically the calcaneus with either the talus or navicular.
Acquired rigid flatfeet may result from failure (stretching) of the plantar ligaments and tibialis posterior tendon (e.g., due to prolonged unaccustomed standing in an older person who has gained a lot of weight). If the plantar calcaneonavicular ligament fails, the head of the talus loses its support and slips inferomedially with flattening of the medial longitudinal arch. For a discussion of acquired adult flatfoot, see http://www.emedicine.com/orthoped/topic461.htm
The skin and subcutaneous connective tissue (superficial fascia) on the dorsum of the foot is thinner and less well innervated than the skin and superficial fascia on the sole of the foot. The superficial fascia on the dorsum is loose, making edema more prominent over this surface when inflammation occurs. The deep fascia over the dorsum is also relatively thin. It is continuous proximally with the inferior extensor retinaculum, which is a thickening of the crural fascia.
The blood supply to the dorsum of the foot is mainly from the dorsalis pedis artery (dorsal artery of the foot) (Gr 5.55A, 5.57B, 5.67B, Table 5.11 [p. 423]; Ne 508, 518, 519, 524). It is the continuation of the anterior tibial artery at the level of a line joining the medial and lateral malleoli. The dorsalis pedis descends just lateral to the extensor hallucis longus tendon, where it is palpated as part of a physical exam in individuals suspected of having peripheral vascular disease. Occasionally a dorsalis pedis pulse is congenitally absent due to the artery’s replacement by an enlarged perforating branch of the fibular artery, which traverses a gap in the lower part of the interosseous membrane to reach the dorsum of the foot (Gr 5.65B). The main branches of the dorsalis pedis are the medial and lateral tarsal branches, arcuate artery, and the terminal division into the deep plantar and first dorsal metatarsal arteries. The tarsal arteries mainly supply structures in the midfoot area.
{kind=link}
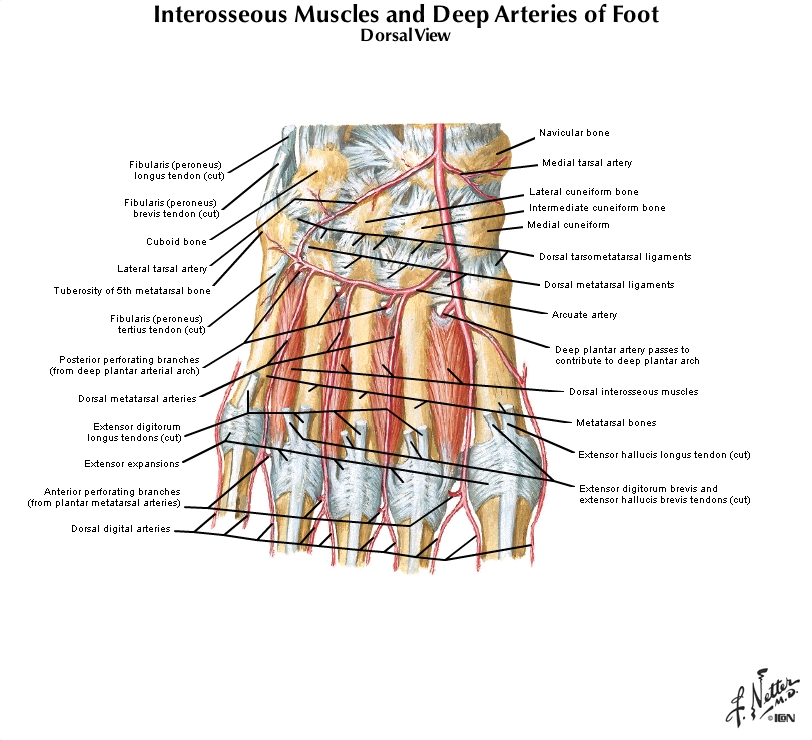
The arcuate artery branches from the dorsalis pedis and arches laterally across the bases of the lateral four metatarsal bones (Gr 5.57B; Ne 519, 524). The arcuate artery gives rise to the second, third, and fourth dorsal metatarsal arteries, which run distally between adjacent metatarsal bones. Each metatarsal artery divides into dorsal digital arteries to the sides of adjacent toes.
The dorsalis pedis ends by dividing into the deep plantar and first dorsal metatarsal arteries (Gr 5.57B, 5.67; Ne 519, 524). The deep plantar artery descends between the heads of the first dorsal interosseous muscle to enter the sole of the foot, where it joins the deep branch of the lateral plantar artery to form the plantar arterial arch. The first dorsal metatarsal artery divides into branches to supply the medial and lateral sides of the great toe and the medial side of the second toe.
The nerve supply to the dorsal region of the foot is mainly by the superficial and deep fibular nerves with a small contribution from the dorsal lateral cutaneous nerve of the foot laterally and the saphenous nerve medially (Gr 5.3A; Ne 471, 530). The superficial fibular nerve leaves the lateral compartment of the leg by piercing the deep (crural) fascia in the distal third of the leg to enter subcutaneous tissue. The superficial fibular nerve divides into medial and lateral branches, which descend and branch to supply skin of most of the dorsum of the foot except the webbing between and adjacent sides of the first and second digits. The deep fibular nerve continues into the dorsum of the foot from the anterior compartment of the leg (Gr 5.54A, 5.55A; Ne 471, 518, 530). It supplies intertarsal joints, the intrinsic muscles on the dorsum of the foot, and the skin of the webbing between the first and second digits as well as their contiguous sides.
The dorsal lateral cutaneous nerve of the foot is the continuation of the sural nerve after it passes the lateral malleolus (Gr 5.3; Ne 471, 472, 530). The dorsal lateral cutaneous nerve of the foot supplies the most lateral hindfoot and midfoot areas on the dorsum. The saphenous nerve is a branch of the femoral nerve that descends along the medial side of the leg with the great saphenous vein. The saphenous nerve may supply skin on the medial side of the foot as far distally as the metatarsophalangeal (MP) joint of the great toe. The superficial fibular nerve supplies the great toe distal to the MP joint.
Unlike the dorsum of the hand, the dorsum of the foot contains two intrinsic muscles, both of which are innervated by the deep fibular nerve (Gr 5.56, 5.58B, 5.59B-C; Ne 509, 518). They are the extensor digitorum brevis and the extensor hallucis brevis, and they are located deep to the tendons of the muscles in the anterior compartment of the leg. The extensor digitorum brevis attaches proximally to the superolateral surface of the calcaneus. It has three small muscle bellies and tendons that insert into the extensor expansions (extensor or dorsal hoods) of toes 2-4 (Gr 5.56B; Ne 518) (Note: some authors describe extensor digitorum brevis tendons inserting into the tendons of extensor digitorum longus). The tendon of the extensor digitorum brevis to digit 5 is usually missing. The extensor digitorum brevis helps the extensor digitorum longus to extend toes 2-4.
The extensor hallucis brevis is actually the medial part of the extensor digitorum brevis but is often listed as a separate muscle. It has a tendon that inserts into the base of the proximal phalanx of the great toe (Gr 5.56B, 5.57A; Ne 518). The extensor hallucis brevis helps the extensor hallucis longus to extend the great toe at the metatarsophalangeal joint.
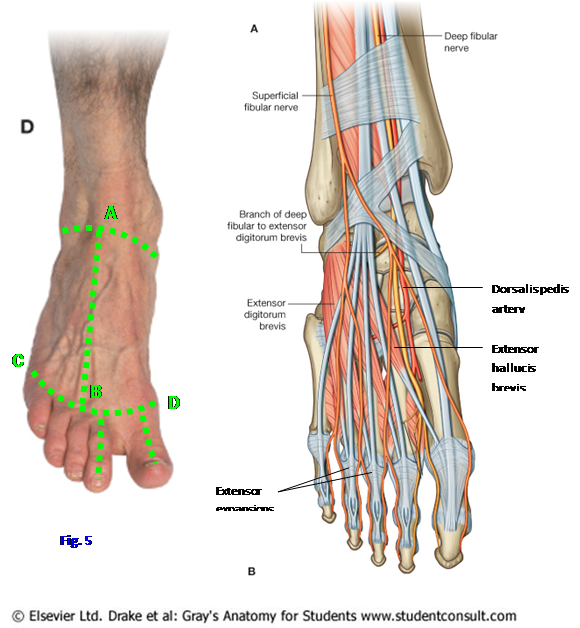
9. Make a longitudinal incision through the skin covering the dorsum of the foot (Fig. 5). Start at the ankle joint and continue down the middle of the foot to the base of the toes (AàB). Make a transverse incision across the foot at the base of the toes (CàD). Reflect the medial skin flap medially toward the great toe side of the foot and the lateral skin flap laterally toward the little toe side. Make an incision down the middle of the great toe and the second toe and reflect or remove the skin.
10. Realize that branches of the superficial fibular nerve supply the skin over most of the dorsum of the foot, but the terminal branches of the deep fibular nerve supply the skin on adjacent sides of the great toe and second toe. The dorsal lateral cutaneous nerve of the foot passes forward from under the lateral malleolus to innervate the lateral side. Attempt to identiry these nerves.
11. Clean the dorsal venous arch located in superficial fascia over the distal portions of the metatarsal bones (Gr 5.5C, 5.6C; Ne 471). Follow the medial continuation of the dorsal venous arch upward into the great saphenous vein and verify that it passes anterior to the medial malleolus. Find the origin of the small saphenous vein from the lateral side of the dorsal venous arch and follow it posterior to the lateral malleolus.
12. Identify the dorsalis pedis artery just lateral to the tendon of the extensor hallucis longus muscle, between it and the tendon of the extensor digitorum longus to the second toe (Fig. 5). Find the terminal division of the dorsalis pedis into the deep plantar and first dorsal metatarsal arteries. Clean the origin of the arcuate artery from the dorsalis pedis medial to the base of the second metatarsal bone. Don’t take time to find its second, third and fourth dorsal metatarsal branches unless the arteries are especially nice examples. If you have difficulty finding the dorsalis pedis, once again find the anterior tibial artery in the anterior compartment of the leg and trace it distally. Be aware that in 3-4% of the population the dorsalis pedis is replaced by an enlarged perforating branch of the fibular artery (Gr 5.65B), which usually is small and anastomoses with the lateral tarsal artery.
13. On the lower extremity on which the superior and inferior extensor retinacula were cut during the leg dissection, displace the tendons of the extensor digitorum longus and fibularis tertius laterally. Clean the extensor digitorum brevis and extensor hallucis brevis muscles. XXX
The thick skin of the sole of the foot is supported by dense superficial fascia. Fibrous septa (retinacula cutis) divide the superficial fascia into fat-filled areas for shock absorption, especially over the heel, and anchor the skin to the deep fascia to improve the “grip” of the sole. The deep fascia of the sole (plantar fascia) has a thick central region with thinner medial and lateral parts, such as was seen in the palm of the hand.
The thick central part of the plantar fascia forms the strong plantar aponeurosis, which corresponds to the palmar aponeurosis of the hand (Gr 5.66B; Ne 520). It consists mainly of longitudinally arranged dense connective tissue fibers. The plantar aponeurosis attaches posteriorly to the calcaneus. Anteriorly it attaches to transverse metatarsal ligaments and through digital bands to the fibrous digital sheaths overlying flexor tendons of the toes. The plantar aponeurosis thus spans the longitudinal arch of the foot and functions as a ligament to help support the arch.
Running and other high-impact activities may result in inflammation of the plantar aponeurosis (plantar fasciitis). Walking when first arising in the morning or after a period of non-weight bearing results in heel pain (e.g., see http://emedicine.medscape.com/article/827468-overview ). Point tenderness may be present near the aponeurosis’ attachment to the medial tubercle of the calcaneus. Chronic inflammation may result in formation of a bone spur at the medial tubercle.
Medial to the plantar aponeurosis the deep fascia is thinner and is labeled the medial plantar fascia (Gr 5.66B; Ne 520). The fascia lateral to the plantar aponeurosis, and also thinner, is the lateral plantar fascia. These deep fasciae form the superficial boundaries for compartments in the sole of the foot that resemble those in the palm of the hand. The plantar aponeurosis overlies the central compartment of the sole. Deep to the central compartment lies an interosseous-adductor compartment containing the metatarsal bones and enclosed by plantar and dorsal interosseous fasciae. Intermuscular septa pass dorsally from the medial and lateral edges of the plantar aponeurosis to the first and fifth metatarsal bones, respectively, to separate the central compartment from the compartment of the great toe and compartment of the small toe. These compartments are important in directing the spread of infection in the plantar portion of the foot. An infection usually spreads along deep fascia rather than eroding through it into adjacent compartments.
The blood supply to the sole of the foot is mainly from the medial and lateral plantar arteries, which are the terminal branches of the posterior tibial artery deep to the flexor retinaculum (Gr 5.67A, Table 5.11 [p. 423]; Ne 522, 523, 524). The medial plantar artery is usually smaller than the lateral plantar artery. They will be discussed in more detail later.
The nerve supply to the skin and superficial fascia of the sole of the foot is from the medial and lateral plantar nerves (Gr 5.3B, 5.66B, Table 5.12 [p. 428]; Ne 521, 522, 529). The medial plantar nerve corresponds in distribution to the median nerve in the hand and is the larger of the two terminal branches of the tibial nerve. It gives rise to three common plantar digital nerves, each of which divides into proper plantar digital nerves to the facing sides of adjacent toes. A separate proper plantar digital branch supplies the medial side of the great toe. The medial plantar nerve innervates skin of the medial part of the sole and the plantar surface of the medial 3½ digits. The smaller lateral plantar nerve supplies skin over the lateral part of the sole and the plantar surface of the lateral 1½ digits via common plantar digital and proper plantar digital branches. It thus corresponds to the ulnar nerve in the hand.
14. Make a transverse incision through the thick skin of the sole of the foot at the base of the toes. Make a longitudinal incision from the middle of the first incision to the middle of the heel and continue up to the cut edge of the skin remaining at the ankle. Remove the flaps of skin. Make a longitudinal incision through the skin of the great toe and at least one other toe. Reflect or remove the resulting flaps of skin.
15. Carefully remove superficial fascia and clean the plantar aponeurosis. Note that it sends digital slips into each of the toes. Preserve and clean the medial plantar nerve as it emerges into superficial fascia medial to the plantar aponeurosis near its mid-length (Gr 5.66B; Ne 520). Find examples of common plantar digital and proper plantar digital branches. Identify the smaller lateral plantar nerve entering subcutaneous connective tissue lateral to the plantar aponeurosis. It has a proper plantar digital branch to the lateral side of the little toe and a common plantar digital branch. Clean them. Find the smaller medial and lateral plantar arteries that accompany the corresponding nerves. XXX
The muscles of the plantar region of the foot may be grouped either by the compartment in which they are located or by the layer in which they are encountered during dissection. Although both approaches offer advantages, learning the muscles of the foot by compartments (functional groups) is probably easier and is also consistent with the way the muscles of the hand are usually studied. When we start the actual dissection of muscles, however, we will do so by layers.
One difference between the human hand and foot is that, although the compartments of the large digit (great toe) and small digit (small or little toe) both contain an abductor and a flexor muscle, neither usually contains an opponens muscle. An opponens occasionally is present in one or both compartments as a variation (e.g., see Anatomy of the Lower Extremity by Debra Draves, 1986, Williams & Wilkins, pp. 297, 299-300) and may contribute to the amazing dexterity with their feet developed by some children born with total (amelia) or partial (phocomelia) absence of the upper extremities.
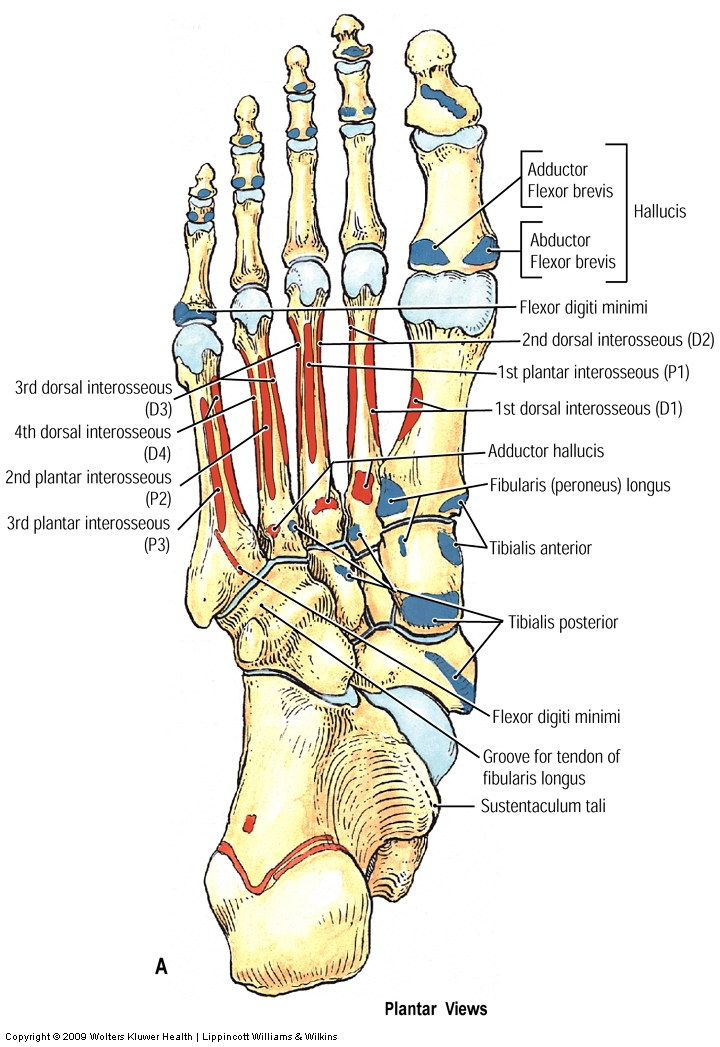
The compartment of the great toe is bounded by the first metatarsal bone, the medial intermuscular septum from the plantar aponeurosis to the first metatarsal, and the medial plantar fascia. This compartment contains two intrinsic muscles of the foot, along with the tendon of the flexor hallucis longus, and is traversed for a short distance by the medial plantar nerve and artery (Gr Tables 5.12-5.15 [pp. 428-431]; Ne 521, 522, 523). The more superficial intrinsic muscle in the compartment of the great toe is the abductor hallucis. It arises from the medial tubercle of the calcaneus and adjacent fibrous connective tissue (e.g., the plantar aponeurosis and flexor retinaculum). The abductor hallucis inserts into the medial side of the proximal phalanx of the great toe with the medial belly of flexor hallucis brevis. The abductor hallucis flexes the metatarsophalangeal (MP) joint of the great toe and slightly abducts it.
The other intrinsic muscle of the great toe is the flexor hallucis brevis (Gr Tables 5.14-5.15 [pp. 430-431]; Ne 521, 522, 523). It arises from the plantar surface of the medial part of the cuboid bone and adjacent lateral cuneiform bone. From this origin it divides into two bellies that pass forward, one on each side of the flexor hallucis longus tendon. The medial belly of the flexor hallucis brevis inserts with abductor hallucis into the medial side of the base of the proximal phalanx. The lateral belly inserts with the adductor hallucis into the lateral side of the base of the proximal phalanx of the great toe. The tendon of each belly contains a sesamoid bone under the head of the first metatarsal bone to help protect against excessive wear. The flexor hallucis brevis flexes the MP joint of the great toe. Both the abductor hallucis and flexor hallucis brevis are innervated by branches of the medial plantar nerve.
The tendon of the flexor hallucis longus traverses the compartment of the great toe between the proximal portions of the abductor hallucis and flexor hallucis brevis en route to its insertion into the distal phalanx. The tendon grooves the under surface of the sustentaculum tali of the calcaneus, crosses diagonally above the tendon of the flexor digitorum longus (Gr 5.64, Table 5.13 [p. 429]; Ne 517, 521, 522), and passes forward between the medial and lateral bellies of the flexor hallucis brevis to enter the great toe. As described with the posterior compartment of the leg, the flexor hallucis longus flexes the great toe and can help plantar flex the foot. It is sometimes said to have a special role in toe-off of the gait cycle, but this is controversial.
The compartment of the small (little) toe is bounded in its distal half by the fifth metatarsal bone, the lateral intermuscular septum from the plantar aponeurosis to the fifth metatarsal, and the lateral plantar fascia. It contains two intrinsic muscles of the foot, the abductor digiti minimi and flexor digiti minimi brevis (Gr Tables 5.12-5.15 [pp. 428-431]; Ne 521, 522, 523). The abductor digiti minimi courses along the lateral border of the foot from a proximal attachment on the tuberosity of the calcaneus and adjacent fibrous structures. It inserts on the lateral side of the base of the proximal phalanx of the little toe. The abductor digiti minimi flexes and slightly abducts the little toe at the metatarsophalangeal (MP) joint.
The flexor digiti minimi brevis is partly hidden by the overlying abductor digiti minimi (Gr Tables 5.14-5.15 [pp. 430-431]; Ne 521, 522, 523). It arises from the base of the fifth metatarsal bone and the fibrous sheath of the fibularis longus tendon. Its insertion is into the lateral side of the base of the proximal phalanx of the little toe with the tendon of the abductor digiti minimi. The flexor digiti minimi brevis flexes the MP joint of the little toe. It is called “brevis” because the longer flexors—flexor digitorum longus and flexor digitorum brevis—also flex the little toe.
The central compartment of the sole is bounded superficially by the plantar aponeurosis and on its deep aspect by plantar interosseous fascia connecting the metatarsal bones. Medially and laterally it is bounded by the medial and lateral intermuscular septa passing deeply from the edges of the plantar aponeurosis to the first and fifth metatarsal bones, respectively. The central compartment contains the flexor digitorum brevis muscle, the tendons of flexor digitorum longus and its associated muscles—quadratus plantae and lumbricals—and the lateral plantar nerve and vessels.
The flexor digitorum brevis muscle lies immediately deep to the plantar aponeurosis (Gr Tables 5.12 [p. 428] and 5.15 [p. 431]; Ne 521). It arises from the medial tubercle of the tuberosity of the calcaneus, from the overlying plantar aponeurosis, and from the medial and lateral intermuscular septa. The muscle typically divides into four tendons, one each for toes 2-5, but the tendon to the little toe may be absent. Opposite the base of the proximal phalanx bone each tendon splits to allow passage of the corresponding tendon of the flexor digitorum longus in its route to the distal phalanx (Gr Table 5.15 [p. 431]; Ne 522). The two slips of the flexor digitorum brevis tendon insert into the middle phalanx of their digit. This arrangement is the same as that of flexor digitorum superficialis and flexor digitorum profundus tendons in the fingers. The flexor digitorum brevis flexes the PIP joints of digits 2-5 and helps to flex the MP joint. It is innervated by the medial plantar nerve.
The flexor digitorum longus tendon runs deep to the flexor digitorum brevis muscle within the central compartment (Gr 5.64A-B, Table 5.13 [ p. 429]; Ne 521, 522). The long flexor tendon enters the compartment diagonally, having passed deep to the flexor retinaculum and the abductor hallucis muscle. In the middle of the foot the tendon divides into four slips, one each for toes 2-5. They enter digital fibrous sheaths with the corresponding tendons of the flexor digitorum brevis muscle. The flexor digitorum longus tendons pass through a split in tendons of the brevis en route to attach to the distal phalanx of their respective digits (Gr Table 5.15 [p. 431]; Ne 522).
Muscles associated with the flexor digitorum longus tendons are the quadratus plantae and four lumbrical muscles (Gr 5.64A, Table 5.13 [p. 429]; Ne 522). The quadratus plantae (flexor accessorius) arises from the medial and lateral sides of the plantar surface of the calcaneus. The two heads join to form a single muscle belly that inserts into the tendon of the flexor digitorum longus near its division into four tendons. Contraction of the quadratus plantae redirects the pull of the flexor digitorum longus from posteromedial to more directly posterior, assisting the flexor digitorum longus in flexing toes 2-5. The quadratus plantae is innervated by the lateral plantar nerve.
The four slender lumbrical muscles resemble those in the hand (Gr Table 5.13 [p. 429]; Ne 522). They take origin from tendons of the flexor digitorum longus and each passes medial to the MP joint to insert into the extensor expansion over the dorsal side of the proximal phalanx. The lumbrical muscles flex the MP joints and theoretically can help extend the PIP and DIP joints at the same time, but their ability to help with extension of the PIP and DIP joints is probably much less than that of the lumbricals in the hand. The first lumbrical is innervated by the medial plantar nerve and the lateral three by the lateral plantar nerve. Note that this innervation pattern is different than in the hand.
The interosseous-adductor compartment lies deep to the central compartment of the sole. It basically is located between dorsal and plantar interosseous fasciae, which enclose the metatarsal bones and contents of the intermetatarsal spaces. The arrangement of the plantar interosseous fascia is more complicated because it also encloses the adductor hallucis muscle (Gr Table 5.14 [p. 430]; Ne 523). The interosseous-adductor compartment contains the adductor hallucis, plantar interosseous muscles, dorsal interosseous muscles, deep branch of the lateral plantar nerve, plantar arterial arch and plantar metatarsal arteries. The muscles of the interosseous-adductor compartment are innervated by the lateral plantar nerve.
The adductor hallucis muscle arises by oblique and transverse heads (Gr Table 5.14 [p. 430]; Ne 523). The oblique head takes origin from the bases of metatarsal bones 2-4 and the sheath of the fibularis longus tendon. The transverse head of the adductor hallucis takes origin from plantar and deep transverse metatarsal ligaments near the third, fourth, and fifth metatarsophalangeal (MP) joints. The oblique and transverse heads of adductor hallucis insert with the lateral belly of the flexor hallucis brevis into the lateral side of the proximal phalanx of the great toe. The adductor hallucis adducts and helps flex the MP joint of the great toe.
Plantar and dorsal interosseous muscles occupy the intermetatarsal spaces (Gr Table 5.15 [p. 431]; Ne 524, 525). The three plantar interossei occupy the second, third, and fourth interosseous spaces. They arise from the bases and medial sides of the third, fourth, and fifth metatarsal bones and cross the MP joints with each inserting into the medial side of the corresponding proximal phalanges. The plantar interossei adduct (PAD = plantar adduct) the third, fourth, and fifth toes (i.e., they move the toes toward the digit of reference in the foot, which is the second toe).
{kind=link}
There are four dorsal interosseous muscles, one in each intermetatarsal interval. They arise from adjacent sides of the metatarsal bones of the space in which they are located. The first dorsal interosseous muscle passes medial to the second MP joint. The second, third, and fourth dorsal interossei pass lateral to the second, third, and fourth MP joints, respectively, to insert into a proximal phalanx. There is only a minor insertion into the extensor expansions, unlike in the fingers. The dorsal interossei abduct (DAB = dorsal abduct) the second, third, and fourth toes.
Lying proximal (posterior) to the interosseous-adductor compartment in the sole, but in the same plane, is the tendon of the fibularis (peroneus) longus muscle (Fig. 6; Gr 5.82, Table 5.15 [p. 431]; Ne 516, 524). It crosses the foot diagonally from lateral to medial in the groove anterior to the tuberosity of the cuboid bone (Gr 5.68A; Ne 511). The tendon inserts into the inferolateral surface of the medial cuboid bone and base of the first metatarsal bone. The fibularlis longus is an evertor of the foot. It acts with the tibialis anterior, which also inserts into the medial cuboid and base of the first metatarsal, to form a sling that probably helps to support the medial longitudinal arch of the foot.
The nerves of the sole of the foot are the medial and lateral plantar nerves, which are terminal branches of the tibial nerve deep to the abductor hallucis muscle (Gr 5.3, 5.66, Tables 5.12 [p. 4.28] and 5.14 [p. 430]; Ne 522, 523, 529). The cutaneous distribution of the medial plantar nerve was described above. The medial plantar nerve supplies motor innervation to four muscles in the foot: abductor hallucis, flexor hallucis brevis, flexor digitorum brevis, and the first lumbrical. All of the other intrinsic muscles of the sole are innervated by the lateral plantar nerve.
The lateral plantar nerve traverses the central compartment diagonally in the fascial interval between the flexor digitorum brevis and quadratus plantae muscles (Gr Table 5.14 [p. 430]; Ne 522). At the lateral margin of the quadratus plantae, the lateral plantar nerve divides into superficial and deep branches. The superficial branch of the lateral plantar nerve branches into a proper plantar digital nerve to skin of the lateral side of the little toe and a common plantar digital branch to supply cutaneous innervation, as previously described. The deep branch of the lateral plantar nerve passes deeper into the sole at the lateral border of quadratus plantae and arches medially across the interosseous-adductor compartment, which lies deep to the central compartment of the sole (Gr Table 5.14 [p. 430]; Ne 522, 523). The deep branch of the lateral plantar nerve accompanies the plantar arterial arch and thus corresponds to the deep branch of the ulnar nerve accompanying the deep palmar arch in the hand. The lateral plantar nerve supplies all of the intrinsic muscles of the sole except the four innervated by the medial plantar nerve.
The lateral plantar artery is the larger of the two terminal branches of the posterior tibial artery (Gr 5.67A; Table 5.11 [p. 423]; Ne 523, 524). It typically is accompanied by two small venae comitantes. The superficial branch of the lateral plantar artery accompanies the superficial branch of the nerve.
The deep branch of the lateral plantar artery sinks into the interosseous-adductor compartment with the nerve and passes medially across the bases of the second, third, and fourth metatarsal bones as the plantar arterial arch (Gr 5.67A; Ne 523, 524). It often is referred to as the “deep plantar arterial arch,” but there usually is no superficial arch in the sole of the foot. The plantar arterial arch is completed medially in the first interosseous space, where it anastomoses with the deep plantar branch of the dorsalis pedis artery.
The plantar arterial arch gives off four plantar metatarsal arteries, each of which divides into two plantar digital arteries to supply the adjacent sides of toes. Perforating branches connect the plantar metatarsal arteries with the dorsal metatarsal arteries. The abundant arterial anastomoses mean that wounds that sever the plantar arterial arch or its larger branches result in severe bleeding. Ligature of the arch is difficult because of its deep position and surrounding structures.16.  AT TABLES 1, 6, 11, 16, 21, 26, AND 31 ON ONE FOOT ONLY, other tissues will be sacrificed to provide an optimal dissection of the arteries and nerves. Locate the posterior tibial artery and tibial nerve within the posterior compartment of the leg just superior to the fibular retinaculum. Using scissors (or a scalpel very carefully!) cut the tissues SUPERFICIAL to the artery and nerve and follow their course into the sole of the foot. If a scalpel is used, protect the artery and nerve by pushing a probe superficial to them before cutting the overlying tissues. Carefully clean and preserve the medial and lateral plantar arteries and nerves and their branches, including the plantar arterial arch. On the other foot, follow the directions below. ____________________________________________________________
AT TABLES 1, 6, 11, 16, 21, 26, AND 31 ON ONE FOOT ONLY, other tissues will be sacrificed to provide an optimal dissection of the arteries and nerves. Locate the posterior tibial artery and tibial nerve within the posterior compartment of the leg just superior to the fibular retinaculum. Using scissors (or a scalpel very carefully!) cut the tissues SUPERFICIAL to the artery and nerve and follow their course into the sole of the foot. If a scalpel is used, protect the artery and nerve by pushing a probe superficial to them before cutting the overlying tissues. Carefully clean and preserve the medial and lateral plantar arteries and nerves and their branches, including the plantar arterial arch. On the other foot, follow the directions below. ____________________________________________________________
17. AT ALL OTHER TABLES, carefully reflect the plantar aponeurosis and remove the medial and lateral plantar fasciae while preserving the cutaneous branches of the medial and lateral plantar nerves and vessels. Cut the plantar aponeurosis anteriorly near the base of the toes where it divides into digital bands and reflect it posteriorly toward the calcaneal tuberosity. This may be difficult due to the attachment of the underlying flexor digitorum brevis to the aponeurosis.
FIRST LAYER OF MUSCLES
18. In the first layer of muscles, from medial to lateral, clean the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi (Gr Table 5.12 [p. 428]; Ne 521). Follow the abductor hallucis to its insertion into the proximal phalanx of the great toe. It inserts together with the medial belly of the flexor hallucis brevis. Clean the flexor digitorum brevis belly and tendons as far as the MP joints. The tendon to the little toe may be missing. Follow the abductor digiti minimi from the tuberosity of the calcaneus to the base of the proximal phalanx of the little toe. Its shared insertion with the flexor digiti minimi brevis probably won’t be apparent at present.
SECOND LAYER OF MUSCLES
19. The second layer of muscles in the sole from medial to lateral is the tendon of the flexor hallucis longus, the tendons of flexor digitorum longus and associated lumbrical muscles, and the quadratus plantae (Gr 5.64A, Table 5.13 [p. 429]; Ne 522).
20. Cut the abductor hallucis and flexor digitorum brevis transversely near their origins and reflect them anteriorly. Clean the tendon of the flexor digitorum longus and follow it forward to its division into four tendons, one each to toes 2-5. Identify the quadratus plantae muscle where it inserts into the lateral aspect of the flexor digitorum longus tendon and follow it back to the tuberosity of the calcaneus. Clean the four lumbrical muscles as they take origin from the tendons of the flexor digitorum longus. Each lumbrical courses anteriorly medial to the tendon of its digit.
21. Incise the fibrous digital sheath along the middle of the second toe. Clean the flexor digitorum brevis tendon where it splits to allow the flexor digitorum longus tendon to pass through toward its attachment on the distal phalanx. Elevate the two flexor tendons and look for slender folds of tissue, short vincula (vincula brevia), passing to them from the phalanges near their insertions. They resemble those in the hand (Gr 6.80B). The long vincula (vincula longa) are variable in the toes. As in the fingers, the vincula carry blood vessels that nourish the flexor tendons.
22. Clean the flexor hallucis longus tendon as it emerges from deep to the flexor digitorum longus tendon and traverses the compartment of the great toe. Don’t follow it to its insertion into the distal phalanx at this time.
23. Trace the medial and lateral plantar nerves and arteries. The lateral plantar nerve and artery pass forward and laterally across the quadratus plantae near its insertion into the flexor digitorum longus tendon. Find the division of the lateral plantar nerve and artery into superficial and deep branches at the lateral border of the quadratus plantae. The cutaneous distribution of the superficial branch of the lateral plantar nerve has already been studied. Note the deep branch of the lateral plantar nerve turning medially to disappear into the interosseous-adductor compartment. Don’t attempt to follow it at this time. The lateral plantar artery likewise divides into superficial and deep branches, and the deep branch will be followed later.
THIRD LAYER OF MUSCLES
24. The third layer of muscles consists of the flexor hallucis brevis, adductor hallucis, and flexor digiti minimi brevis (Gr Table 5.14 [p. 430]; Ne 523). To expose this layer, cut the quadratus plantae at its origin from the calcaneus and reflect it forward. Now cut the common tendon of the flexor digitorum longus as it enters the foot and turn it forward with the quadratus and lumbrical muscles.
25. Clean the flexor hallucis brevis muscle but leave the flexor hallucis longus tendon intact. Follow the medial belly of the flexor hallucis brevis to a common insertion with abductor hallucis into the medial side of the base of the proximal phalanx of the great toe. Clean the lateral belly of the flexor hallucis brevis to its insertion into the lateral side of the base of the proximal phalanx. Note that the lateral belly inserts with the adductor hallucis muscle.
26. Clean the oblique and transverse heads of the adductor hallucis. Follow them until they join and insert with the lateral belly of the flexor hallucis brevis into the proximal phalanx of the great toe.
27. Find and clean the flexor digiti minimi brevis. It is smaller that the abductor digiti minimi and partially hidden by it. Finding the flexor’s tendon of insertion—it inserts with the abductor into the proximal phalanx of the little toe—and following the muscle proximally to its origin may be easier. It takes origin from the base of the fifth metatarsal bone and the fibrous sheath of the fibularis longus tendon.
28. IN ONE FOOT clean the plantar arterial arch and the accompanying deep branch of the lateral plantar nerve. To expose these structures, detach the origin of the oblique head of the adductor hallucis and reflect it forward toward its insertion. Clean the plantar metatarsal arteries branching from the plantar arch. Attempt to find the deep plantar artery emerging from the first intermetatarsal space between the heads of the first dorsal interosseous muscle to complete the arch medially.
FOURTH LAYER OF MUSCLES
29. DO NOT attempt a complete dissection of the three plantar interosseous and four dorsal interosseous muscles. Instead, IN ONE FOOT, IN THE FOURTH INTERMETATARSAL SPACE (i.e., between the fourth and fifth digits), find the insertions of the third plantar and fourth dorsal interosseous muscles on the proximal phalanx of the fifth toe and the fourth toe, respectively. To do this use scissors or a scalpel to cut the transverse head of the adductor hallucis and the transverse metatarsal ligaments between the heads of the fourth and fifth metatarsal bones and pry them slightly apart. Clean the attachment of the third plantar interosseous muscle on the medial side of the proximal phalanx of the fifth toe followed by that of the fourth dorsal interosseous on the lateral side of the proximal phalanx of the fourth toe.
FINALLY
30. Before leaving the foot, study the attachments of two muscles that help to support the arches of the foot, the tibialis posterior tendon and the fibularis longus tendon (Fig. 6; Gr 5.64A-B, 5.82A; Ne 516, 523, 524). The tibialis posterior’s main insertion is into the tuberosity of the navicular bone, but slips of the tendon insert also into the cuneiform bones, cuboid and the bases of metatarsal bones 2-4.
31. Trace the tendon of the fibularis longus muscle from the cuboid bone at the lateral border of the foot across the sole to its insertion into the medial cuneiform and base of the first metatarsal bone. It has a fibrous sheath partially formed by the long plantar ligament (Gr 5.82A; Ne 516). XXX
The illustrations in this dissection guide are used with permission from Gray’s Anatomy for Students. 2005, by Richard Drake, Wayne Vogel, and Adam Mitchell, Elsevier Inc., Philadelphia; and from Grant’s Atlas of Anatomy, 11E, 2005, Anne Agur and Arthur Dalley II, Lippincott Williams & Wilkins, Philadelphia.