Thoracic Wall, Pleura, and Lungs
The thorax is the part of the trunk connecting the neck and abdomen. It consists of the thoracic wall enclosing the thoracic cavity. The thoracic cavity communicates with the neck superiorly through the superior thoracic aperture, which is bounded by the superior border of the manubrium, the first pair of ribs and their costal cartilages, and vertebra Tv1. The thoracic cavity is separated from the abdominal cavity inferiorly by the diaphragm, a musculotendinous sheet that has a major function in respiration and fills the inferior thoracic aperture (Gr 1.9, 2.1; Ne 179, 187, 190). The diaphragm is not a flat structure; rather, it domes superiorly into the thorax. Additionally, it has a posterior attachment that is more inferior than its anterior attachment (Gr 1.25A; Ne 256).
The thoracic skeleton is formed by the sternum, the 12 pairs of ribs and associated costal cartilages, and the 12 thoracic vertebrae and intervening intervertebral discs(Gr 1.9A; Ne 179). The sternum consists of a superior manubrium, flattened body, and small inferior xiphoid process (Gr 1.10). The manubrium and body of the sternum meet at an easily palpable sternal angle, where the second costal cartilages articulate. The xiphisternal joint is the junction between the body and xiphoid process of the sternum. The sternal angle is clinically useful in counting ribs and forms an important landmark for determining the surface projections of thoracic organs. The xiphisternal joint indicates the level of the inferior border of the heart and the superior border of the liver.
Study the parts of a typical rib (Gr 1.11; Ne 179, 180). It has a head, neck, tubercle,and shaft (body). The shaft of the rib articulates anteriorly with a costal cartilage at the costochondral junction. On the shaft of the rib the costal angle is the site where the rib both bends sharply forward and twists slightly. Observe the costal groove along the inferior surface, which protects the intercostal nerve and vessels. The ribs articulate posteriorly with vertebrae.
The costal cartilages form joints anteriorly either with the sternum or with another costal cartilage. The costal cartilages of ribs 1-7 articulate directly with the sternum (and are called “true ribs”), but those of ribs 8-12 don’t (and are called “false ribs”). The costal cartilages of ribs 8-10 articulate with the cartilage above, but the 11th and 12th ribs end anteriorly among muscles of the body wall (and are also called “floating ribs”). The intercostal spaces between adjacent ribs are filled by three layers of intercostal muscles and their associated blood vessels and nerves (Gr 1.18; Ne 185).
1. Study the thoracic skeleton. Identify the manubrium, body, xiphoid process, sternal angle, and xiphisternal joint of the sternum. Study the head, neck, tubercle, and shaft of a typical rib. On the shaft find the costal angle and the costal groove.
2. Turn your attention to the supine cadaver. The pectoralis major and minor muscles were reflected previously. Now cut the anterior attachments of the serratus anterior muscle from the upper 5-6 ribs and reflect them posteriorly, trying to retain some lateral cutaneous branches of intercostal nerves (Gr 6.15, 6.24, 6.26; Ne 243, 414). XXX
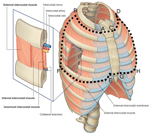
3. Dissect at least two intercostal spaces on each side. Cut the inferior attachment of the external intercostal muscle and external intercostal membrane between the sternum and the midaxillary line and reflect them superiorly. Be careful to avoid cutting into the second layer, the internal intercostal muscle. XXX
Cutting and reflecting the external intercostal muscle will expose the internal intercostal muscle (Gr 1.17, 1.18, Table 1.1 [p. 21]; Ne 183, 185). In the anterior thoracic wall its fibers course inferolaterally at right angles to those of the external intercostal. Internal intercostal muscle fibers occupy the intercostal space from the sternum anteriorly to the angles of the ribs posteriorly. From the angles of the ribs to the vertebrae, the internal intercostal muscle is replaced by an internal intercostal membrane (Gr 1.18; Ne 185).
4. In the same intercostal spaces where the external intercostal muscle was reflected, cut the inferior attachment of the internal intercostal muscle between the lateral border of the sternum and the midaxillary line and reflect it superiorly. Be careful to avoid cutting too deeply, into the third and deepest layer, the innermost intercostal muscle.
5. Near the midaxillary line, the neurovascular structures are larger and easier to identify than they are more anteriorly. Probe the superior part of the fascial plane between the reflected internal intercostal muscle and the innermost intercostal muscle to find the intercostal vein, artery, and nerve, which are arranged, fromsuperior to inferior in this interval (Gr 1.16, 1.17, 1.18; Ne 225). Often, the intercostal vein and artery are hidden in the costal groove. Except for the first two intercostal spaces, the posterior intercostal arteries are branches of the thoracic aorta (Gr 1.18, 1.70C, 1.77; Ne 185, 225). Most of the posterior intercostal veins are tributaries of the azygos system of veins (Gr 1.73, 1.74, 1.75; Ne 186, 224). Intercostal nerves are the anterior rami of thoracic spinal nerves (Gr 1.18, 1.77, 1.78; Ne 185). XXX
Due to the characteristic superior position of the larger neurovascular structures in an intercostal space, a needle is inserted or an incision is made above the superior border of the lower rib bounding the space to access the thoracic cavity (e.g., for procedures such as thoracocentesis). This threatens only smaller collateral branches, although they are avoided too if possible.
6. Study the innermost intercostal muscles deep to the neurovascular bundle. Innermost intercostal muscle fibers have an orientation similar to that of the internal intercostal muscle, of which they often are considered a deep part.
7. Turn your attention to the anterior part of the intercostal space. Carefully remove the intercostal muscles and membranes from the medial part of the third, fourth, and fifth intercostal spaces (i.e., from the sternum to about 5 cm lateral to the sternum). Find the internal thoracic artery and vein descending just lateral to the sternum. The internal thoracic artery is a branch of the first part of the subclavian artery. It gives rise to small anterior intercostal arteries that pass laterally to anastomose with the posterior intercostal arteries (Gr 1.18, 1.19; Ne 183, 184, 185).
REMOVING THE ANTERIOR THORACIC WALL
8. The next step is to remove the anterior thoracic wall to expose the contents of the thoracic cavity. Use scissors to carefully cut through the intercostal muscles and membranes of the first and sixth intercostal spaces on both sides of the body starting next to the sternum and extending laterally to the midaxillary line (Fig. 7-1, A to B, C to D, and E to F, G to H). Be careful not to cut into the underlying lung. Next, use a Stryker saw to make a transverse cut across the manubrium at the level of the first intercostal space (Fig. 7-1, A to C). Make the second transverse cut across the sternum through the articulations of the sixth costal cartilages near the xiphisternal junction (Fig. 7-1, E to G). Now saw vertically through the second to sixth ribs on each side at the level of the midaxillary line or just anterior to it (Fig. 7-1, B to F, C to H). Lift the anterior thoracic wall away from the body by separating it with your fingers from the adherent underlying parietal pleura.
9. Study the internalsurface of the anterior thoracic wall (Gr 1.20; Ne 184). The transversus thoracis muscles are 4-5 bands of muscle on each side passing superolaterally from the posterior surface of the lower part of the sternum to costal cartilages 2-6. These bands of muscle lie posterior to the lower part of the internal thoracic vessels and hold them against the anterior thoracic wall. Look for the upper 5-6 anterior intercostal arteries, which branch from the internal thoracic artery. Find the terminal division of the internal thoracic artery into superior epigastric and musculophrenic arteries. The superior epigastric artery traverses a small gap in the diaphragm to enter the anterior abdominal wall (Gr 2.5; Ne 185, 249). The musculophrenic artery passes along the superior surface of the anterior attachment of the diaphragm, giving off the lower anterior intercostal arteries.
10. Set aside the anterior thoracic wall and start your examination of the thoracic contents. The thoracic cavity contains the right and left lungs, each enclosed within its own pleural sac within a pulmonary cavity, separated by a median partition of tissue, the mediastinum (Gr 1.21, 1.22, 1.23, 1.24, 1.25,1.26; Ne 187, 190, 191, 192, 205). XXX
The median mass of tissue between the right and left pulmonary cavities is the mediastinum (Gr 1.25; Ne 210 [no image]). The mediastinum is subdivided into a superior mediastinum and an inferior mediastinum. The boundary between them is a transverse plane connecting the sternal angle with the intervertebral disc joining vertebrae Tv4/Tv5. The inferior mediastinum is further subdivided with reference to the heart and pericardium. The heart and its enclosing pericardium comprise the middle mediastinum. The anterior mediastinum lies between the pericardium and sternum, and the posterior mediastinum is posterior to the pericardium and the downwardly sloping diaphragm, in front of the vertebral column.
Each lung invaginates a closed serous sac, the pleura (Gr 1.24B; Ne 190, 191, 192). The visceral pleura is the layer of pleura that adheres to the lung and faithfully follows its contours (Gr 1.24B, 1.25C; Ne 210 [no image]). The parietal pleura is the layer of pleura that lines the internal surface of the thoracic wall, the superior surface of the diaphragm, and the mediastinum. A potential space, the pleural cavity, contains a small amount of serous fluid between the visceral and parietal layers of pleurae. Adhesions may develop between the visceral and parietal pleurae during life due to inflammation (pleurisy, pleuritis). Such adhesions produce pain during exertion. Even in the absence of adhesions, the roughness of the pleural surfaces resulting from pleurisy produces a pleural friction rub detectable with a stethoscope.
The parietal pleura is subdivided into the parts that line the ribs (costal pleura), the diaphragm (diaphragmatic pleura), and the mediastinum (mediastinal pleura). A dome of parietal pleura that projects through the superior thoracic aperture into the root of the neck is called the cervical pleura, or pleural cupula (Gr 1.24B-C; Ne 190). It is important to recognize that a penetrating wound in the root of the neck may tear the cervical pleura, allowing air to enter the pleural cavity (pneumothorax) and causing the lung to collapse.
Recesses of the pleural cavity, which are not filled by the lungs except during the deepest inspirations, are found inferiorly between the costal and diaphragmatic parietal pleura (costodiaphragmatic recess) and anteriorly between the costal and mediastinal parietal pleura (costomediastinal recess) (Gr 1.21, 1.24, 1.68; Ne 190, 191). Fluid (serous fluid, pus, blood) may accumulate in the costodiaphragmatic recess in upright patients with pathological conditions or following injury. It may have to be removed with a hypodermic needle (thoracocentesis) or by insertion of a chest tube.11. Study the parts of the parietal pleura and explore the pleural recesses with your hands. Blood or other body fluids that enter the pleural cavity in injury or disease accumulate in the costodiaphragmatic recess in upright patients. Notice that the left parietal pleura deviates away from the body of the sternum in the region of the fifth intercostal space, forming a shallow notch (Gr 1.22, 1.26A; Ne 190).
This pleural notch and the corresponding cardiac notch in the left lung allow insertion of a needle into the pericardium (e.g., to drain fluids from the pericardial cavity [pericardiocentesis]) without entering the pleural cavity or damaging the lung. The area of the pericardium exposed by the pleural and cardiac notches is the bare area of pericardium.
12. The lungs will now be removed intact for study. Use your hands to explore the entire pleural cavity around each lung, tearing any adhesions that you find between visceral and parietal pleurae. The mediastinal pleura is continuous with the visceral pleura around structures entering and leaving the lung (root of the lung). Notice an inferior extension of pleura from the root of the lung to the diaphragm (pulmonary ligament) (Gr 1.29, 1.30; Ne 193). Carefully tear the pulmonary ligament. Now place an index finger and thumb around the root of the lung within the pleural cavity to ensure that the root has been fully mobilized. If you have difficulty with this, ask an instructor for assistance. Cut the root of the lung in the middle of the mobilized area with large scissors or a scalpel, taking care not to damage the lung. Remove the lung. Perform the same procedure with the opposite lung.
13. With the lungs removed, again examine the subdivisions of the parietal pleura lining the pulmonary cavity. Between the mediastinal pleura and fibrous pericardium, anterior to the cut root of the lung on each side, identify the phrenic nerve and the accompanying small pericardiacophrenic vessels (Gr 1.21, 1.75; Ne 205). Clean and preserve these structures. XXX
Each phrenic nerve (C3,4,5) is the sole motor innervation to its half of the diaphragm (hemidiaphragm), and bilateral phrenic nerve lesions result in respiratory paralysis. That is why patients with spinal cord injuries at or above the C4 level usually don’t survive without respiratory assistance. The phrenic nerve also supplies sensation to all but the periphery of the diaphragm. Therefore, the origin of the phrenic nerves from the cervical spinal cord provides the basis for sensations produced by irritation of the diaphragmatic pleura or peritoneum by thoracic or abdominal disease (e.g., from inflammation of the gallbladder) to be “felt” by the patient in the shoulder region in the C3, 4 dermatomes (referred pain).
THE RIGHT LUNG
14. Study the right lung. It has three lobes—superior, middle, and inferior—demarcated by horizontal and oblique fissures (Gr 1.21, 1.27, 1.29; Ne 190, 193, 195). If the individual had experienced inflammation of the pleurae during life (pleurisy/ pleuritis), the visceral pleura of adjacent lobes may adhere, obscuring the fissures. Break any adhesions that may be present to define the horizontal and oblique fissures. Palpate the lung. Even embalmed normal lung tissue usually has a spongy, if slightly soggy, texture. If you feel small hard nodules or large firm areas, a disease process was likely present. Are there mottled, dark areas of accumulated carbon particles? Even non-smokers who live in an industrialized society often exhibit these. Are thin-walled, air-filled blebs apparent? These are an indication of the breakdown of the internal structure of the lung (walls of alveoli, alveolar ducts) in emphysema, reducing the surface area for gas exchange between air and blood.
15. Study the mediastinal surface of the right lung (Gr 1.29; Ne 193). Structures that make up the root of the lung enter and leave at the hilum. Identify the division of the primary bronchus into secondary (lobar) bronchi. Each lobar bronchus divides into tertiary (segmental) bronchi to bronchopulmonary segments, which are independent functional units of the lung. The right lung has 10 bronchopulmonary segments (Gr 1.31; Ne 196, 197). XXX
A diseased bronchopulmonary segment can be surgically removed while leaving the surrounding lung tissue functioning normally (segmentectomy).
Bronchi can easily be identified by the presence of stiff hyaline cartilage in their walls. The secondary bronchus to the superior lobe of the right lung is the only one in either lung that lies above the accompanying branch of the pulmonary artery, and so is given the special name “eparterial bronchus.” All of the other bronchi in both lungs are hyparterial bronchi.
At the hilum the pulmonary artery typically lies anterior and superior to the bronchus and divides into branches that accompany the bronchi (Gr 1.28C; Ne 193). The pulmonary veins are usually anterior and inferior in position at the hilum (Gr 1.28A, 1.29; Ne 193, 200). Unlike the bronchi and pulmonary artery branches, the larger tributaries of the pulmonary veins occupy intersegmental positions and are used as surgical landmarks during segmentectomies. Remember that pulmonary arteries carry blood from the right ventricle of the heart to the lungs to be oxygenated, and pulmonary veins return the oxygenated blood from the lungs to the left atrium.
16. Look for small arteries that follow the posterior surface of the bronchi into the right lung. These branches of the right bronchial artery supply oxygen to the tissues of the lung itself (Gr 1.63, 1.70C; Ne 201, 231). There is only one right bronchial artery, which has a variable origin, but often branches from the third right posterior intercostal artery.
17. An embalmed lung usually retains contact impressions made by adjacent structures, and these contact impressions are useful in understanding spatial relationships in the thoracic cavity. On the rounded costal surface of the right lung look for grooves made by the ribs (Gr 1.22, 1.27). The inferior diaphragmatic surface of the lung is concave due to the right dome of the diaphragm, which is raised over the liver (Gr 1.29, 2.19, 2.21A; Ne 190, 193, 264). On the mediastinal surface of the right lung, look anterior to the hilum for the concavity of the cardiac impression (Gr 1.29; Ne 193). Extending superiorly from it is the groove for the superior vena cava, which continues into the groove for the right brachiocephalic vein. Above the hilum find the groove for the arch of the azygos vein (Gr 1.29, 1.73, 1.74,1.75; Ne 193, 224). Behind the hilum lies the groove for the esophagus. Another impression that may be more difficult to identify is the groove for the right subclavian artery, which arches across the apex of the lung (Gr 1.22; Ne 187, 193).
THE LEFT LUNG
18. Turn your attention to the left lung. It has two lobes—superior and inferior—separated by the oblique fissure (Gr 1.27, 1.30; Ne 190, 193). Break any adhesions between visceral pleura of the superior and inferior lobes to define the oblique fissure. Note the cardiac notch in the anterior border of the superior lobe resulting from protrusion of the apex of the heart to the left side. The small, tongue-like process that borders the cardiac notch inferiorly is the lingula. The lingula corresponds to the middle lobe of the right lung.
19. On the mediastinal surface of the left lung, at the hilum, find the primary bronchus dividing into two secondary bronchi. Unlike the right lung, the left lung is often described as having only 8 bronchopulmonary segments due to the fusion of two segments in each lobe. The general arrangement of structures of the root of the lung at the hilum is the same as in the right lung: bronchus posterior, pulmonary artery anterior and superior, and pulmonary veins anterior and inferior. There are two left bronchial arteries arising from the thoracic aorta to supply tissues of the left lung (Gr 1.63, 1.70C; Ne 201, 231). Attempt to find these small arteries on the posterior surface of the bronchi.
20. Study the contact impressions on the left lung. On the mediastinal surface find the cardiac impression, which is larger than the impression on the right lung because two-thirds of the heart lies to the left of the midline (Gr 1.22, 1.30; Ne 193). Above the hilum identify the groove for the arch of the aorta and behind the hilum the groove for the descending thoracic aorta. Passing upward from the arch of the aorta find the groove for the left subclavian artery crossing the apex of the lung (Gr 1.22, 1.30; Ne 193). Anterior to the lowest part of the groove for the descending aorta, look for a small esophageal impression. This is created by the esophagus as it inclines to the left just before traversing the diaphragm, but the impression may be indistinct (Gr 1.69, 1.76; Ne 200, 225, 226). XXX
The illustrations in this dissection guide are used with permission from Gray’s Anatomy for Students. 2005, by Richard Drake, Wayne Vogel, and Adam Mitchell, Elsevier Inc., Philadelphia; and from Grant’s Atlas of Anatomy, 11E, 2005, Anne Agur and Arthur Dalley II, Lippincott Williams & Wilkins, Philadelphia.